WHO Executive Board urges intensified efforts to give world one less infectious disease to worry about and work towards sustainability of ga...
While tremendous progress has been made in the fight against polio, wild poliovirus remains endemic to two countries and the threat of cVDPV...
For a few incredible eradicators, a life’s purpose doesn’t stop at retirement
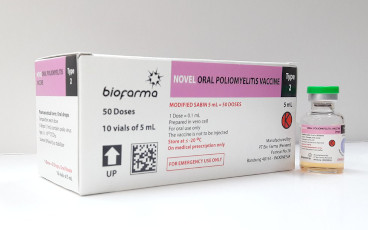
The recommendation further advances nOPV2 as a critical new tool in the fight against circulating vaccine-derived poliovirus type 2 (cVDPV2)
Report outlines the vital role that the polio eradication network plays in global health security and argues that this infrastructure must b...
Dr. De Sousa has spent more than twenty years charting the highs and lows of polio eradication in Angola.
WHO has issued an Emergency Use Listing recommendation for the type 2 novel oral polio vaccine (nOPV2)
Nouvel outil à utiliser pour lutter contre le PVDVc2
We talk to Dr Wadood about the impact of COVID-19 on the global polio eradication effort, and how the polio infrastructure is supporting COV...
Integrated polio and measles campaign protects thousands of children.
Melissa Corkum, Polio Outbreak Response Senior Manager for UNICEF, has dedicated a large part of her professional life to ending polio.
Personnel from the country’s long-running polio programme have been trained to detect COVID-19 cases.
Meet the experts who deploy at a moment’s notice to fight outbreaks across the region.
Exploring the ‘plus’ in PolioPlus.
Long commutes and cold box in hand, no place is too far away in the fight to end polio
In Mogadishu, the capital of Somalia, dedicated environmental surveillance teams search for the poliovirus in the city’s drains.
A unique look at immunization efforts in a sprawling water community
Women are ensuring that the children in Papua New Guinea are protected and vaccinated
Following confirmation of circulating vaccine-derived poliovirus type 2 (cVDPV2) on 8 January 2019, planning for an outbreak response is und...
Jean-Marc Olivé, Chairman of the Technical Advisory Group, reflects on what needs to be done to end polio in the Horn of Africa.
To truly ensure no child is left behind, the Global Polio Eradication Initiative is reaching out to some of the most remote communities in t...
Mohamed Shire, a polio eradication expert from Somalia, speaks about lessons from a life tirelessly working to eradicate first smallpox, the...
Dr Mohammad Al Safadi, Technical Officer for Polio Outbreak Preparedness and Response, WHO HQ, talks to us about the tactics and strategies...
A review committee met in Nairobi to assess progress of the African region towards being certified polio-free
After an 18-month long intensive vaccination campaign in the face of a poliovirus outbreak in Syria, the outbreak has been successfully stop...