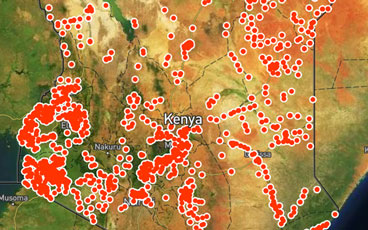
In the Horn of Africa, health workers are using application-based technology to respond to poliovirus outbreaks with greater speed and accur...
Papua New Guinea’s first polio case in decades is a champion for eradication
Special report on Papua New Guinea
In a complex environment, partners of the polio programme are working to vaccinate every child.
Darcy Levison, WHO Polio Eradication Officer, speaks to us about the logistical challenges of reaching every single child with polio vaccine...
The innovations making a difference to outbreak response.
Take a look at how the Papua New Guinea Government, the World Health Organization, and partners of the Global Polio Eradication Initiative a...
Government launches emergency measures to prevent children from lifelong paralysis.
In the sahel surrounding Lake Chad, health workers provide vaccines to refugees and internally displaced people.
Outbreak response to be launched to stop further spread of the virus
The Ministry of Foreign Affairs of the Republic of Korea announced today an additional US$ 2 million to fund polio outbreak response and sur...
In Iraq, polio vaccinators work to protect conflict-affected children.
In January, children in Raqqa city received polio vaccines for the first time in two years as families return to the devastated city.
Why we are developing new polio vaccines for the post-eradication era.
La Dre Adele Daleke Lisi Aluma s’efforce d’atteindre les enfants jamais vaccinés
In Nigeria, experts from the frontline of polio eradication are helping to end other disease outbreaks.
In Somalia, determined women are the face of polio eradication.
Dr Adele Daleke Lisi Aluma works to reach children who have never been vaccinated
In at-risk areas of Chad, large-scale polio campaigns are increasing the immunity of every child.
The strong polio eradication infrastructure in Borno is supporting Nigeria to vaccinate over eight million people against yellow fever.
Hans Everts, long time polio eradicator, shares personal stories from the frontline of outbreak response, and explains how the lessons learn...
All hands on deck to stop polio in Syria amidst conflict
In Afghanistan, blood tests are identifying where vaccination campaigns are working, and where gaps remain to be filled.
Community health workers responding to humanitarian crisis in Nigeria are helping to stop polio and malaria hand in hand.
One of an animated series on the global drive to eradicate polio.