A series on the ‘plus’ in PolioPlus: preventing other diseases
Long commutes and cold box in hand, no place is too far away in the fight to end polio
Despite juggling several hats, women have greatly improved the quality and outcome of polio campaigns. Read their testimonials.
Grassroots efforts got Nigeria over the barriers to polio vaccination
Update on polio eradication efforts in Pakistan for July 2019
Vaccination and religious dialogue
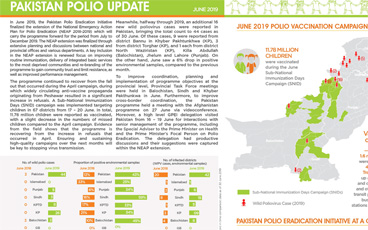
Update on polio eradication efforts in Pakistan for June 2019
Update on polio eradication efforts in Pakistan for May 2019
A unique look at immunization efforts in a sprawling water community
Reaching underserved populations with immunization in the Niger Delta
Everyday people in Pakistan advocating for vaccinations
Update on polio eradication efforts in Pakistan for April 2019
Papua and West Papua provinces rise to challenges of stopping polio
All travellers crossing the border between Pakistan and Afghanistan are vaccinated against polio, regardless of age
Update on polio eradication efforts in Afghanistan for February 2019
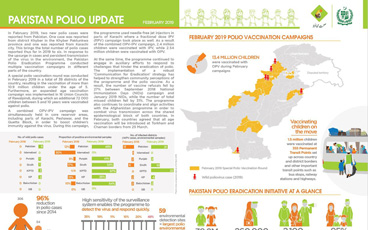
Update on polio eradication efforts in Pakistan for February 2019
Resilience and resolve are the keywords for women eradicating polio
On International Women’s Day, we celebrate the role of women in the polio eradication efforts in Pakistan
Women health workers and have been highly effective in polio eradication efforts, often as the only point of contact in rural settings.
A look at some of the women in Somalia’s polio programme
Surveillance officer at WHO pushes through gender-related obstacles to help end polio in Pakistan
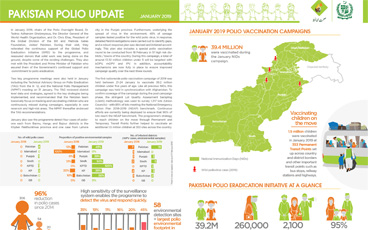
Update on polio eradication efforts in Pakistan for January 2019
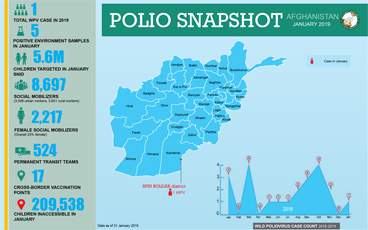
Update on polio eradication efforts in Afghanistan for January 2019
On the road to polio eradication in Pakistan.