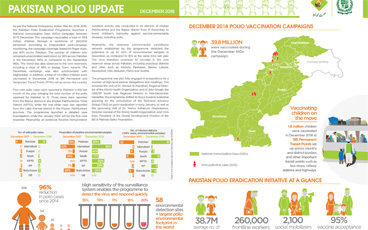
Update on polio eradication efforts in Pakistan for December 2018
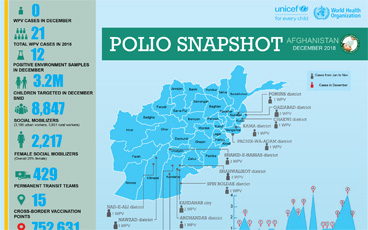
Update on polio eradication efforts in Afghanistan for December 2018
Following confirmation of circulating vaccine-derived poliovirus type 2 (cVDPV2) on 8 January 2019, planning for an outbreak response is und...
As the Global Polio Eradication Initiative (GPEI) enters its 31st year, the Chairs of the effort’s main global advisory bodies issue an extr...
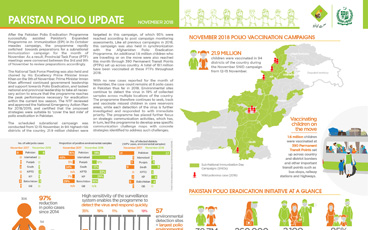
Update on polio eradication efforts in Pakistan for November 2018
In the Horn of Africa polio outbreak, immunization efforts are focusing on a group known as “special populations”.
Early analysis of campaign data points to a successful vaccination round in a polio-free country at risk of possible importation.
After an 18-month long intensive vaccination campaign in the face of a poliovirus outbreak in Syria, the outbreak has been successfully stop...
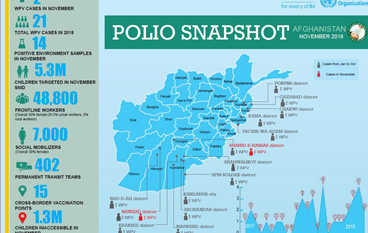
Update on polio eradication efforts in Afghanistan for November 2018
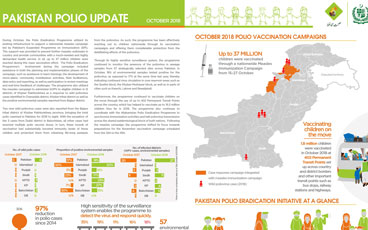
Update on polio eradication efforts in Pakistan for October 2018
What did we learn?
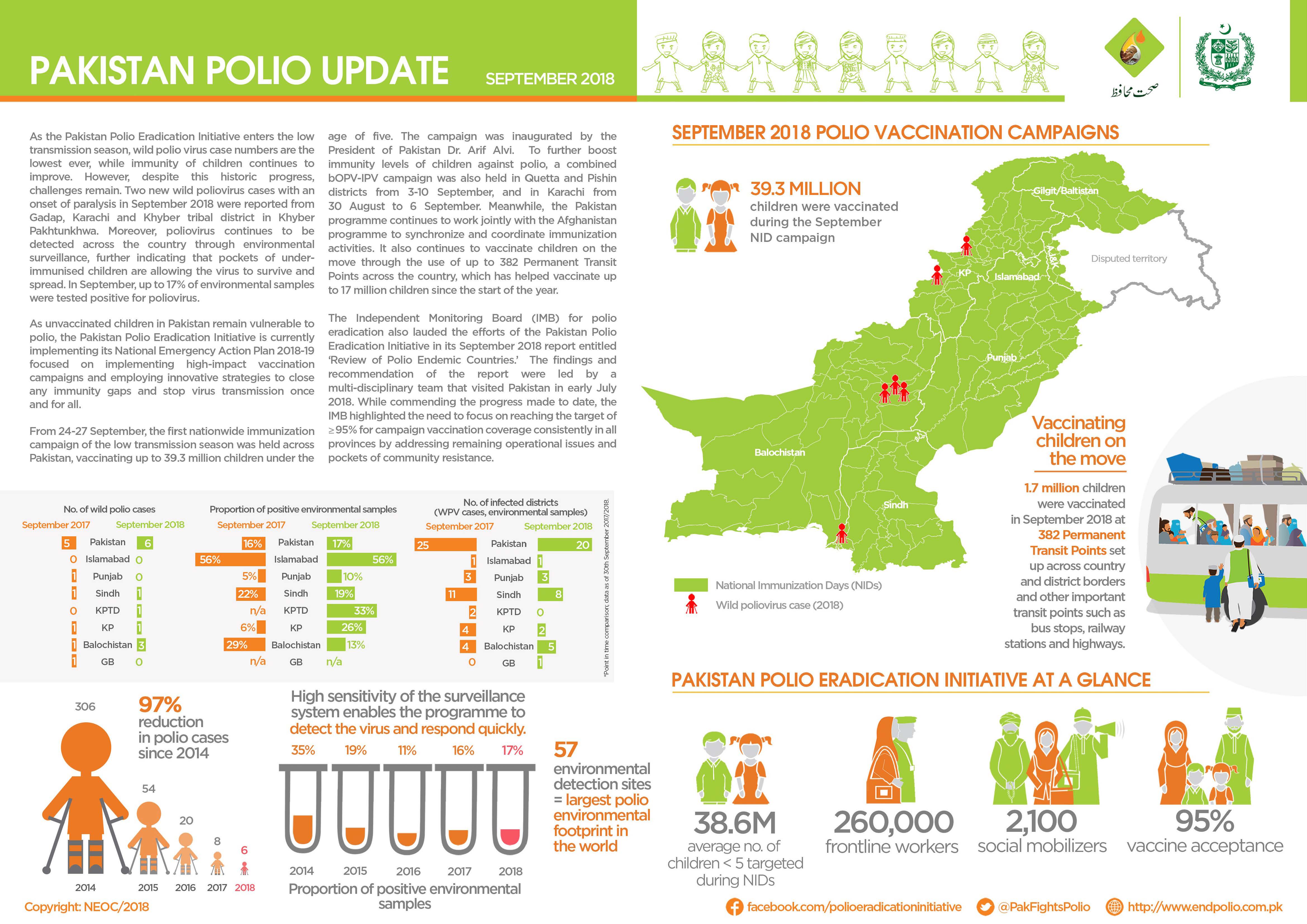
Update on polio eradication efforts in Pakistan for September 2018
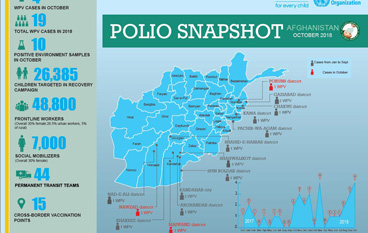
Update on polio eradication efforts in Afghanistan for October 2018
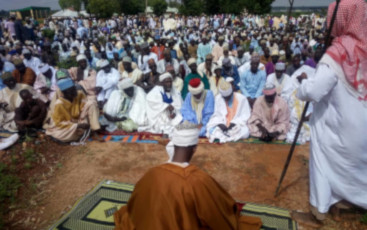
Religious clerics promote routine immunization and other health services by delivering messages to husbands, fathers and sons at mosques.
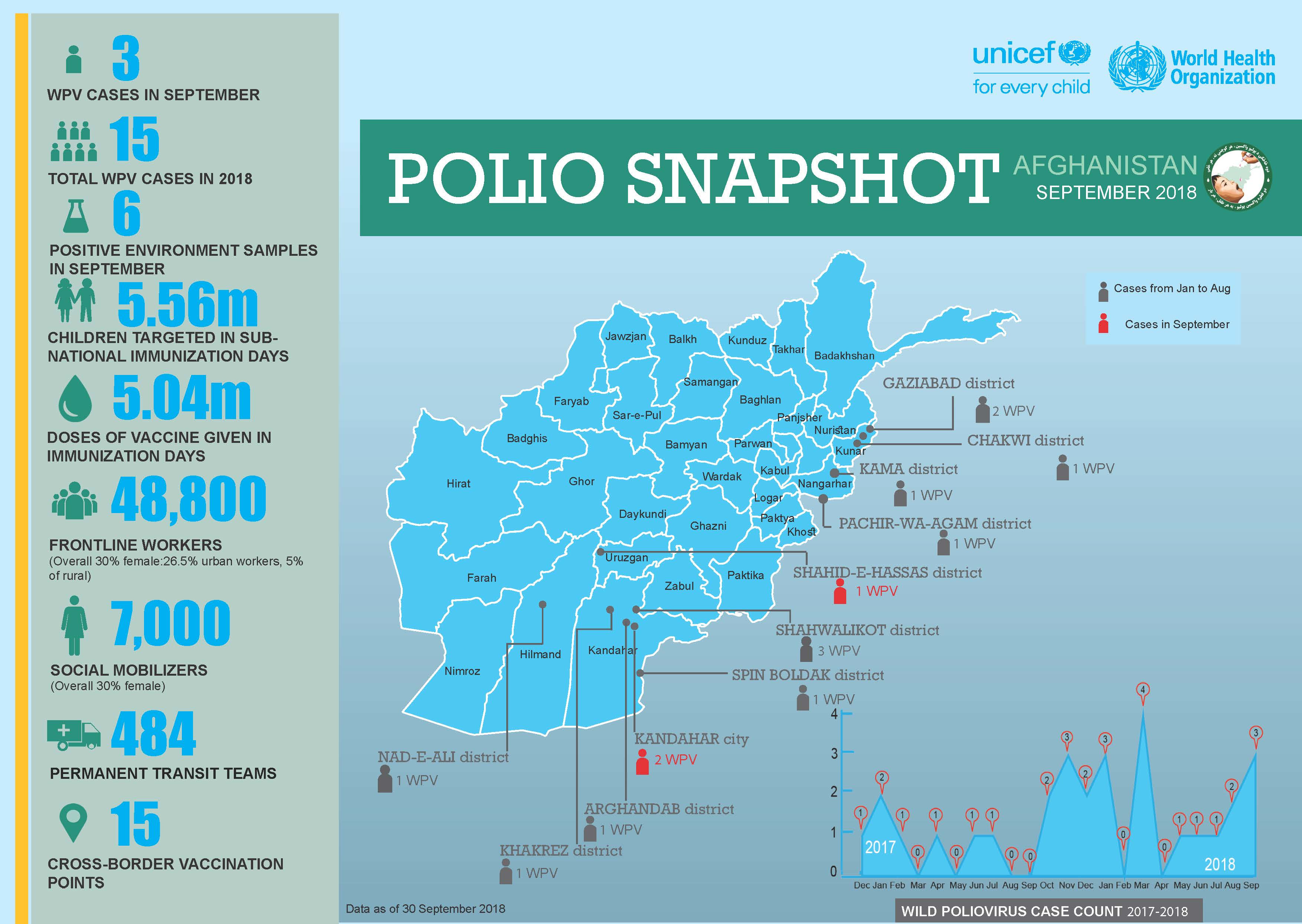
Update on polio eradication efforts in Afghanistan for September 2018
Meet a religious leader helping to end polio in Pakistan.
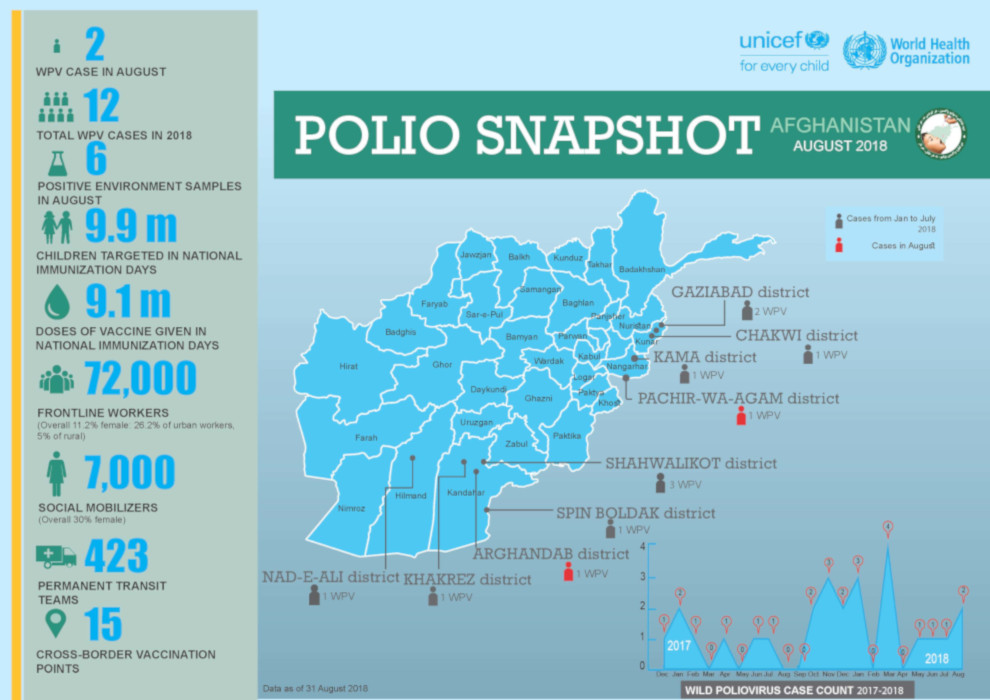
Update on polio eradication efforts in Afghanistan for August 2018
In a complex environment, partners of the polio programme are working to vaccinate every child.
UNICEF community mobilizers engage mothers and fathers to ensure that every child is safe from polio.
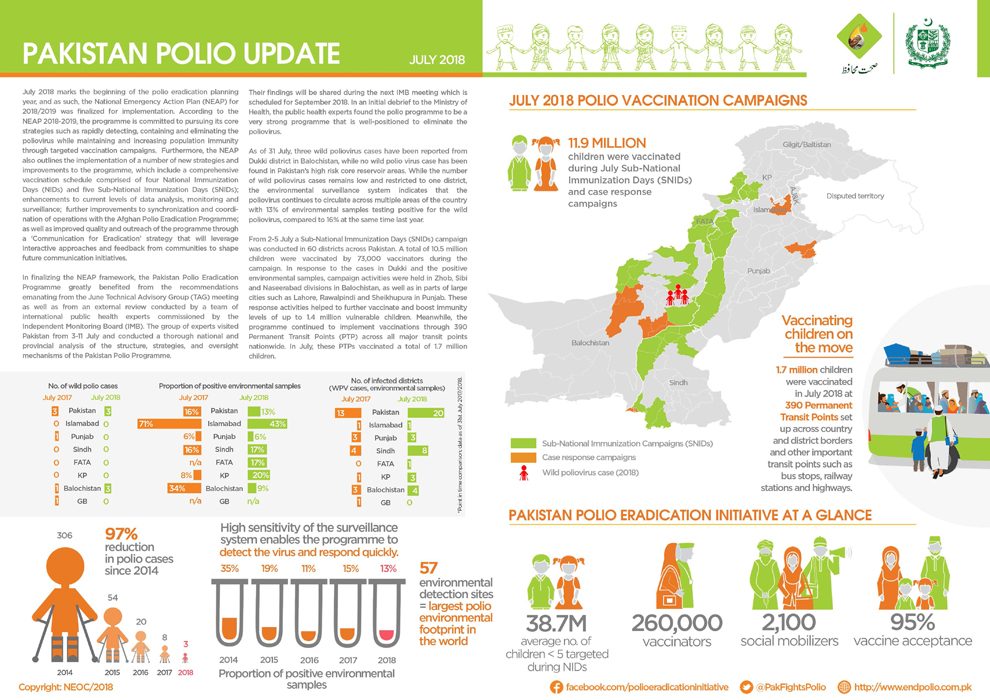
Update on polio eradication efforts in Pakistan for July 2018
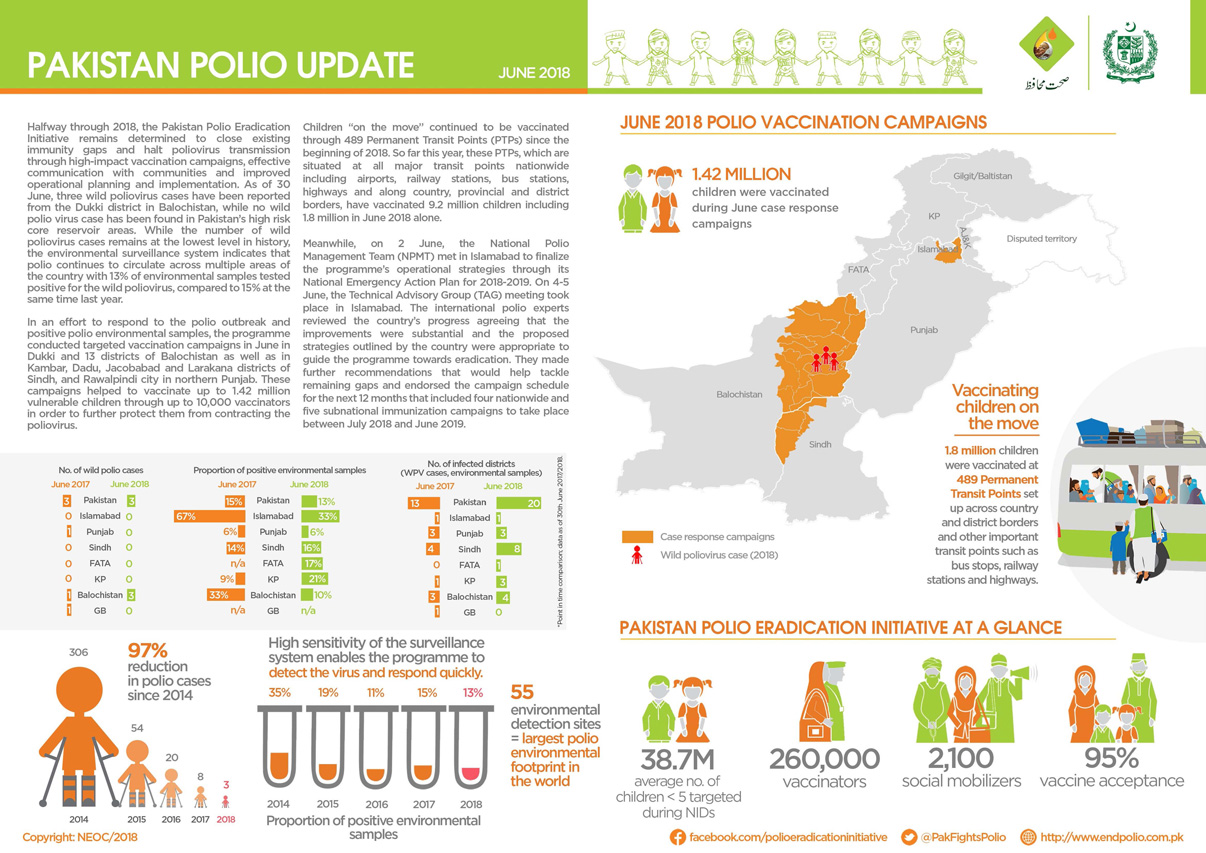
Update on polio eradication efforts in Pakistan for June 2018
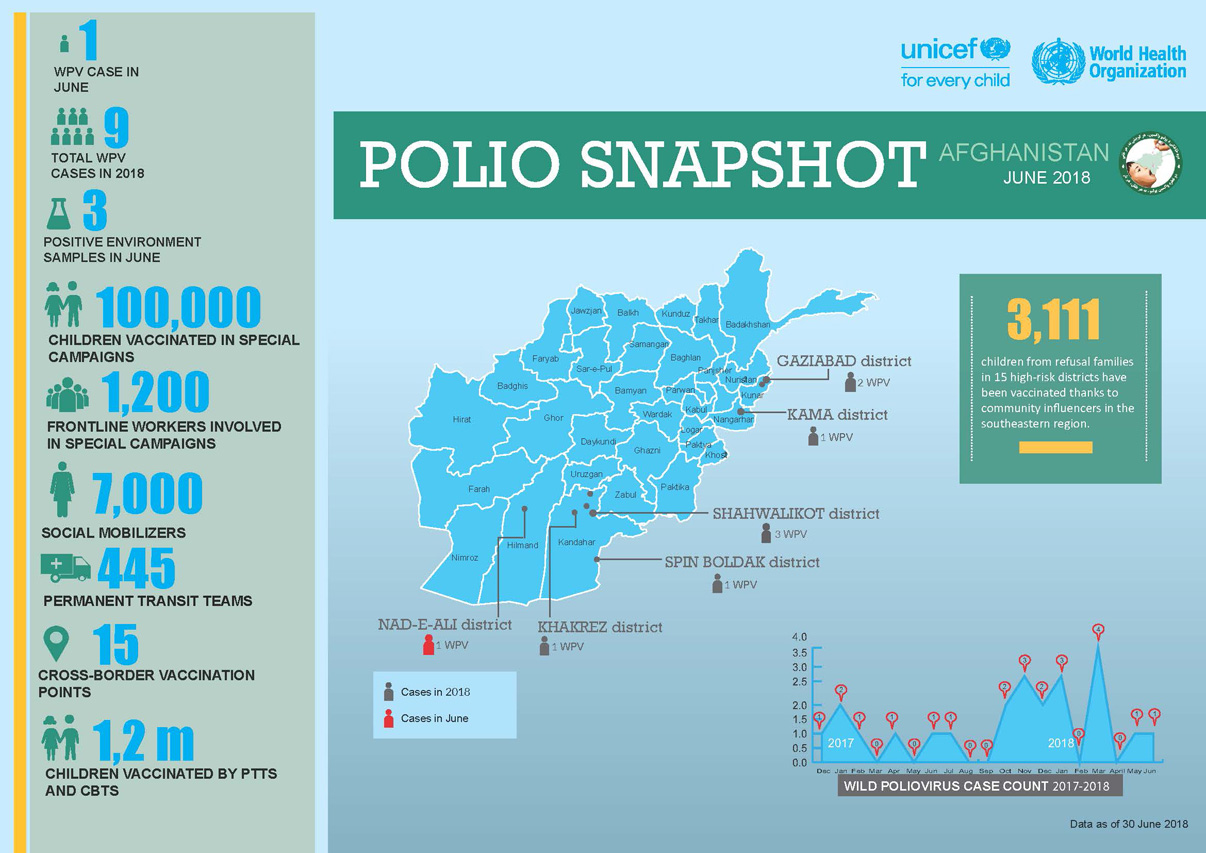
Update on polio eradication efforts in Afghanistan for June 2018
Afia is part of one of the biggest female work forces in Afghanistan.
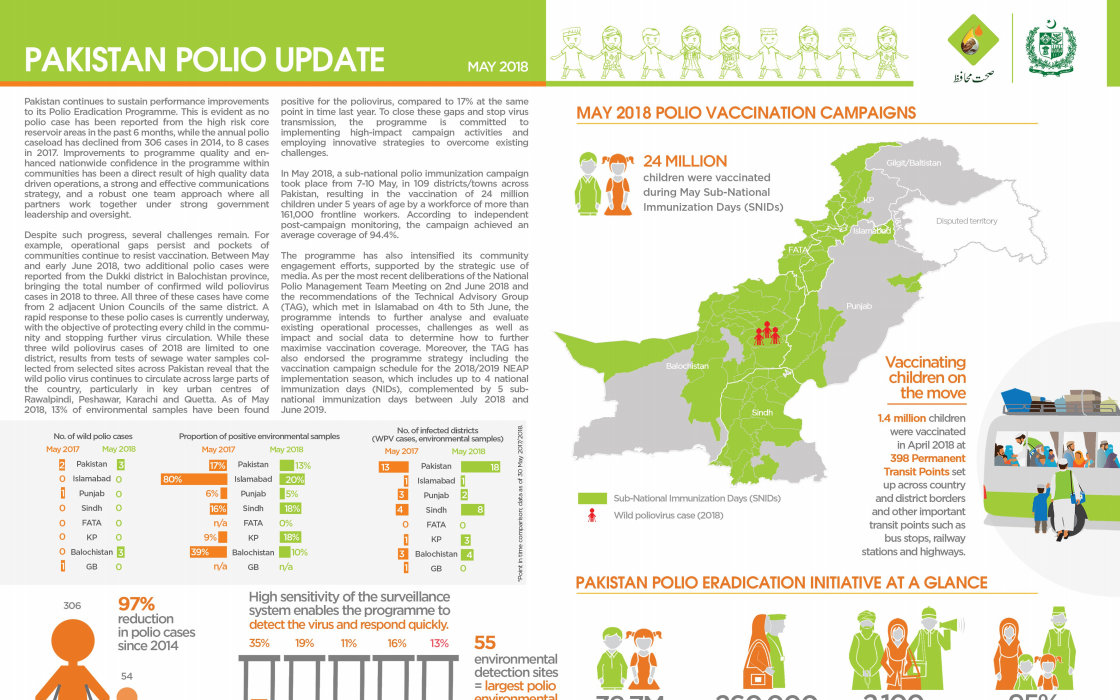
Update on polio eradication efforts in Pakistan for May 2018
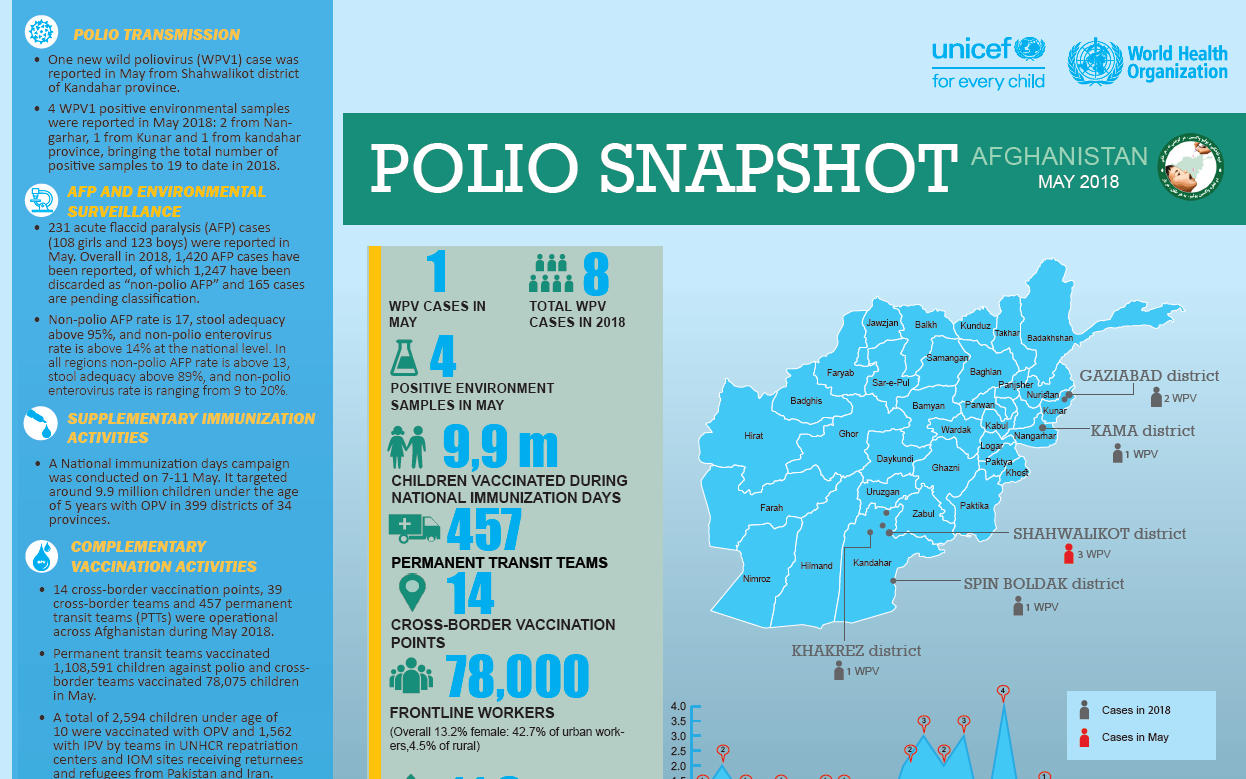
Update on polio eradication efforts in Afghanistan for May 2018