With polio at the lowest levels in history in Pakistan, the country is about to launch an all-out and hopefully final assault on the disease in 2018. To help these emergency efforts, the Government of Germany announced today an additional € 2 million in financial support, to Pakistan’s national emergency action plan. Germany is a longtime supporter of the Global Polio Eradication Initiative (GPEI) with contributions totaling more than US$ 550 million to the effort, not including a recently announced additional pledge of € 19.9 million to Nigeria’s polio eradication effort for 2018. For its engagement in polio eradication, including in fostering global commitment, Germany has on numerous occasions been internationally recognized at the highest levels. Chancellor Angela Merkel is a past recipient of Rotary International’s prestigious Polio Champion Award.
The Global Polio Eradication Initiative partners would like to extend their profound gratitude to both the Government of Pakistan and Germany for their collaboration and for their tremendous support and engagement in the effort to eradicate polio globally.
The year’s end offers the chance to reflect on the polio programme’s milestones and challenges in 2017, and look ahead to what we can achieve in the coming year. 2017 saw the fewest wild polio cases in history — a total of 17 cases, or a 50% reduction from the year before—with these cases occurring in just two countries: Afghanistan and Pakistan. Yet the need to reach every last child is more important than ever, as demonstrated by surveillance gaps in Nigeria and outbreaks of vaccine-derived polio in Syria and the Democratic Republic of the Congo.
From programme strategies that helped protect progress and overcome obstacles, to commitments from donors and partners, 2017 demonstrated the resolve required to achieve a polio-free future. Accelerating progress in the new year and ending polio for good will require maintaining these political and financial commitments as well as building upon the programme’s efforts to find the virus wherever it exists.
Rooting out the virus
Throughout 2017, developments in disease surveillance – both in humans and in the environment – allowed the programme to better hone in on the virus and identify its remaining hiding places.
These innovations are building robust, sensitive surveillance networks around the world that pick up every trace of the virus and enable the programme to develop targeted immunisation responses before polio has the chance to paralyse children.
The year also came with new challenges, including outbreaks of circulating vaccine-derived polio in Syria and the Democratic Republic of the Congo, where conflict has ravaged the health infrastructure. In these communities, and others where polio still exists, difficult terrain, conflict and highly mobile populations can all stand as hurdles to vaccinating children. Yet the polio programme continues to find new and effective ways of delivering vaccines.
For example, in Afghanistan, a collaboration with a mobile circus is sharing important messages about polio vaccination with hard-to-reach populations, including those living in camps for internally displaced persons. In Pakistan, campaigns based at border crossings and train stations vaccinated children on the move who might otherwise have been missed by traditional methods. And in Syria, dedicated workers are delivering vaccines at transit points and registration centres for internally displaced persons. Thanks to these strategies, more than 255,000 children have been vaccinated in Deir Ez-Zor, 140,000 were reached in Raqqa and the programme continues to work to reach every child.
The mobile circus passed on vital health care and social messages, encouraging full immunization of every child. UNICEF Afghanistan / Ashley Graham
Renewed commitment to end the disease
Complementing these programmatic innovations were political and financial commitments that highlighted polio eradication as a priority for global health leaders. These included:
Next year, country programmes will need to continue working to ramp up surveillance, particularly in Nigeria, and reach children everywhere with vaccines. Cross-border coordination between Pakistan and Afghanistan, which has already had a huge impact in reducing cases, will continue to be critically important to stopping transmission.
At the same time, the global community is beginning to solidify plans for keeping the world polio-free once eradication is achieved. Countries are developing strategies for transitioning the infrastructure and tools that they currently use to fight polio. And the GPEI is working with global stakeholders and partners to develop the Polio Post-Certification Strategy, which will define the activities needed to keep polio from returning after the virus is eradicated.
If the remaining endemic countries continue to do all that they can to stop the virus, and if the global community continues to meet the level of political and financial commitment needed to make and keep children everywhere polio-free, 2018 will bring the world’s best opportunity yet to end the disease.
Despite focused efforts to stop the transmission of wild poliovirus in 2017, to date this year 17 cases have been reported globally; six from Pakistan and 11 in Afghanistan. During a series of meetings to review progress in the two endemic countries, which make up one epidemiological block, members of the Technical Advisory Group (TAG) on polio eradication concurred that while both Pakistan and Afghanistan continue to make progress, continued transmission threatens gains already made towards interruption.
The TAG meetings, held in Islamabad and Kabul, recognized the efforts of both countries to coordinate activities closely, focusing on clearly identifying missed children, the reasons they have been missed, and putting in place operational plans to overcome these challenges. Efforts made to adjust national emergency action plans and build on the lessons learned from previous years and other countries have been commended by expert members of the TAG and hailed as key drivers behind the momentum.
TAG however reminded the country programmes of the remaining gaps and concluded that consistently reaching and vaccinating high-risk mobile population groups is essential if Afghanistan and Pakistan are to interrupt transmission over the coming months.
Ongoing transmission threatening the end game
The greatest risk to polio eradication, according to TAG chair Jean Marc Olive, are the reservoirs that continue to harbor the virus: the northern corridor comprising of eastern Afghanistan and Greater Peshawar – Khyber in Pakistan, the southern corridor linking southern Afghanistan (Kandahar and Hilmand) with Quetta block, Balochistan province, in Pakistan and Pakistan’s economic hub, Karachi.
Recognizing the already high level of Government commitment from both countries, TAG insisted that sustained leadership at all levels in both countries would be essential for the implementation of recommendations, including maintaining coordination at the national, provincial and district levels, as well as among the bordering districts in the common corridors of transmission.
Specific recommendations for addressing areas with continued transmission included the development of joint Action Plans for the common reservoirs (northern and southern corridors) linking the two endemic countries ’ as well as to strategize for improving program implementation quality in other high risk areas as well as among the high risk mobile populations.
About the Technical Advisory Group
The Technical Advisory Group (TAG) was established to review progress towards polio eradication in specific countries, assess implementation of previous TAG recommendations, discuss planned activities and issue recommendations to address constraints facing national programmes in achieving their targets. TAG meetings are attended by country-specific TAG members, national representatives and partner organizations, both international and regional.
“I feel our collective productivity has improved manifold, ever since we started working together with the Community Based Vaccinators from the polio eradication programme,” says Syed Mussayab Shah, a tone of pride in his voice. Shah is a vaccinator with the Expanded Programme of Immunization, posted at Gulbahar Civil Dispensary, Peshawar district, Khyber Pakhtunkhwa. He is responsible for immunizing children against nine vaccine-preventable childhood diseases.
Reaching children with vaccines in dense urban environments can be a significant challenge. So the polio eradication programme and the team responsible for delivering routine vaccines – the Expanded Programme on Immunization – are working together to make sure that they do the job as best they can, explains Shah. “We are determined to reach and vaccinate every child in our area. And to ensure this, we exchange information and notes with the community based vaccinators twice every week.”
“The synergy between the two programmes has been a blessing as we are reaching more children with vaccination every day, including those living in urban slums. Our spirits are high and we are determined to reach every last child.” Dr Akram Shah
Vaccination challenges in urban areas
Where families live in concrete housing units in urban slums, access to health care is a persistent challenge. The urban slums are often unrecognized, lack essential infrastructure and are low priority for local health authorities. This translates into low and unequitable coverage of social services in urban areas – including vaccination.
Pakistan is the most urbanized country in South Asia and the population living in urban slums continues to increase. The urban population has risen from an estimated 43 million in 1998 to 73 million in 2014. In Peshawar, increased migration is an additional challenge, making it the sixth biggest city in the country.
The challenge of identifying and vaccinating children living in urban areas, especially those living in slums and migrant families, is demanding innovation and skill sharing. The teamwork between the polio eradication team and the Expanded Programme for Immunization is ensuring everyone benefits – especially children who urgently need the protection offered by vaccines.
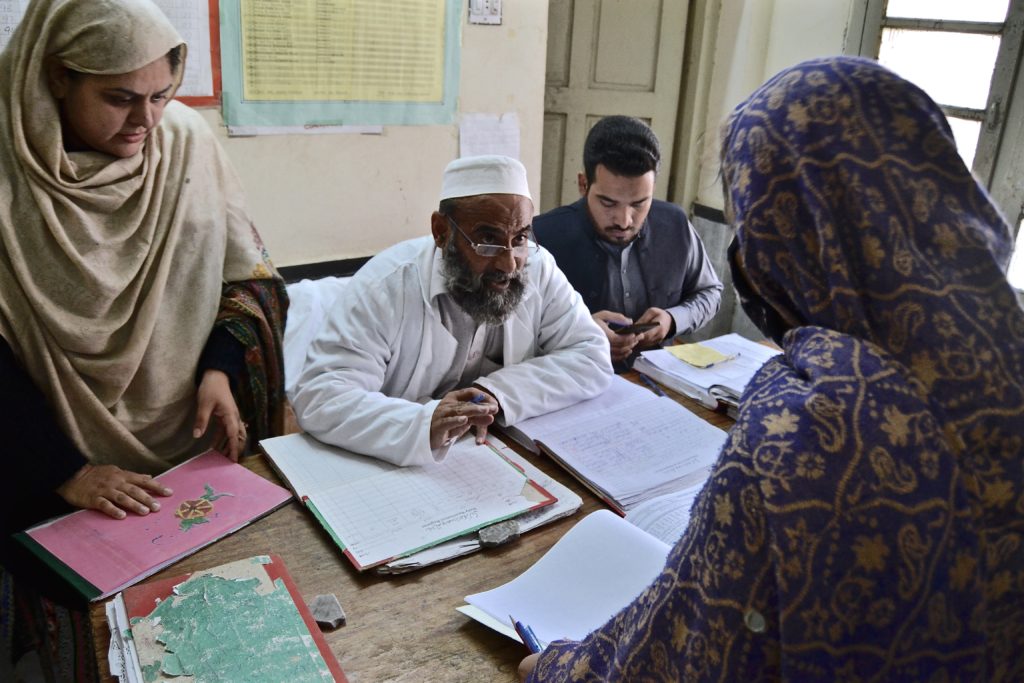
Increasing vaccination coverage through collaboration
The Civil Dispensary is the only government health facility in the area that caters not only to the residents of Gulbahar but also those living in adjoining slums. Community-based polio vaccinators from local areas come to this health facility to sit side by side with their colleagues from the broader vaccination programme to review their field books containing the housing maps and vaccination details of every single child under five in their areas. Microplans, containing this detailed information of local communities, are a valuable tool of the polio eradication programme. From this essential information, routine vaccinators make a list of unvaccinated children for follow-up who might be falling through the cracks. The polio vaccinators also refer clients from their communities to the health facility to receive their other routine vaccines. This collaboration is game changing for the drive to protect every last child against vaccine preventable disease.
UNICEF, with funding from Gavi, the Vaccine Alliance, is supporting the Government of Pakistan in improving routine immunization coverage in urban slums with a focus on seven major cities in Pakistan in collaboration with the polio eradication programme.Referring to the synergy initiative, Shah says, “Earlier we worked without defined plans and targets. Now, due to the information sharing from community based polio vaccinators, we have plans with identified areas and targets that help us monitor our own progress as well as the vaccination coverage.”
“Record keeping of families in urban slums is a very difficult job,” shares Tabassum Shuaib, a polio community-based vaccinator from Peera Gaib, Peshawar.
Teamwork paying off
“Families are constantly moving in and out from here – and many of those that move in do not have a vaccination card. They can only recall the number of times their child has been vaccinated. However, now I have all the families, pregnant mothers and children under five from this community registered and their data is maintained at the Gulbahar Civil Dispensary, so we can keep track ourselves and make sure no child is missed.”
Dr Akram Shah, Director of the Expanded Programme of Immunization in the area, is pleased with the rewards of this teamwork: “Peshawar offers the same challenges as any other major city of Pakistan. With increased migrant population and urbanization during the past decade, the burden of ensuring access to basic life and health resources to all has also increased. The synergy between the two programmes has been a blessing as we are reaching more children with vaccination every day, including those living in urban slums. Our spirits are high and we are determined to reach every last child.”
Nine-year old Adil Khan comes from Peshawar, Pakistan’s sixth largest city and capital of Khyber Pakhtunkhwa province. He is the oldest of the four children of Shami Ullah, a local laborer who often struggles to make ends meet. Together with his wife and four children, he lives in Wahid Ghari, a poor area of Peshawar, where many other underprivileged families reside.
If Shami Ullah’s life wasn’t difficult enough already, Adil was diagnosed with polio in 2008, only 5 months after he was born. After a couple of days of high fever followed by weakness in his left leg, Shami Ullah rushed his baby to the hospital where Adil was tested for polio. Unfortunately, the test came back positive. “We had heard about polio before, so when we learnt our son had it, we were very worried,” Shami Ullahsaid. “I just didn’t want to accept that Adil would not be able to walk his entire life.”
Adil’s story is not unique. In 2008, 21 children in Peshawar were diagnosed with polio, while there were a total of 117 cases reported that year in Pakistan. So far this year, there have been only five cases of wild poliovirus reported in Pakistan, down from 20 last year and 54 in 2015. The recent progress has been the result of strong government commitment, support and oversight at every level, strengthened programme performance and broad community acceptance.
Polio is a crippling and potentially deadly infectious disease caused by the virus which invades the nervous system and can cause irreversible paralysis. For polio victims, this has often meant lifelong social exclusion. However, Adil can walk and goes to school, thanks to the support of orthotic devices and physiotherapy. “We are so happy to see our eldest son run. He is just like other children,” Adil’s father said.
The rehabilitation story of Adil is one of almost 700 stories of children who have been provided with rehabilitation services by Pakistan’s Polio Rehabilitation Initiative. The initiative, which started in 2007, initially provided support to children from Pakistan’s province of Khyber Pakhtunkhwa and Federally Administered Tribal Areas. In November 2011, the programme increased its span to almost all parts of Pakistan.
“This initiative of provision of rehabilitation services to polio affected children is an important combination of medical and social rehabilitation,” said Dr Maryam Mallick who heads the Polio Rehabilitation Initiative with WHO Pakistan. When a child is paralyzed with polio, a rehabilitation officer visits the home of the polio patient to assess the needs. On the basis of this assessment, rehabilitation plans for both medical and social rehabilitation are being developed. The medical services include provision of orthotic devices, surgical procedures, physiotherapy, as well as regular follow-up services.
There are many benefits to rehabilitation to these children – with the right treatment children not only improve mobility, but they gain independence and allow them to enroll in school. “To ensure the regular attendance of the child, the educational expenses for the yearly tuition fee, uniform, books, shoes, and even a small amount for pocket money is being given to the principal of the respective school instead of being given to the parents,” Dr. Mallick said.
Adil is currently a second grade student at the Peshawar Cambridge Public School. He likes to study, which makes his father proud. “When he grows up, I would like him to become a doctor so that he can help people in need,” said Shami Ullah, who is also now a strong advocate of the Polio Eradication Initiative.
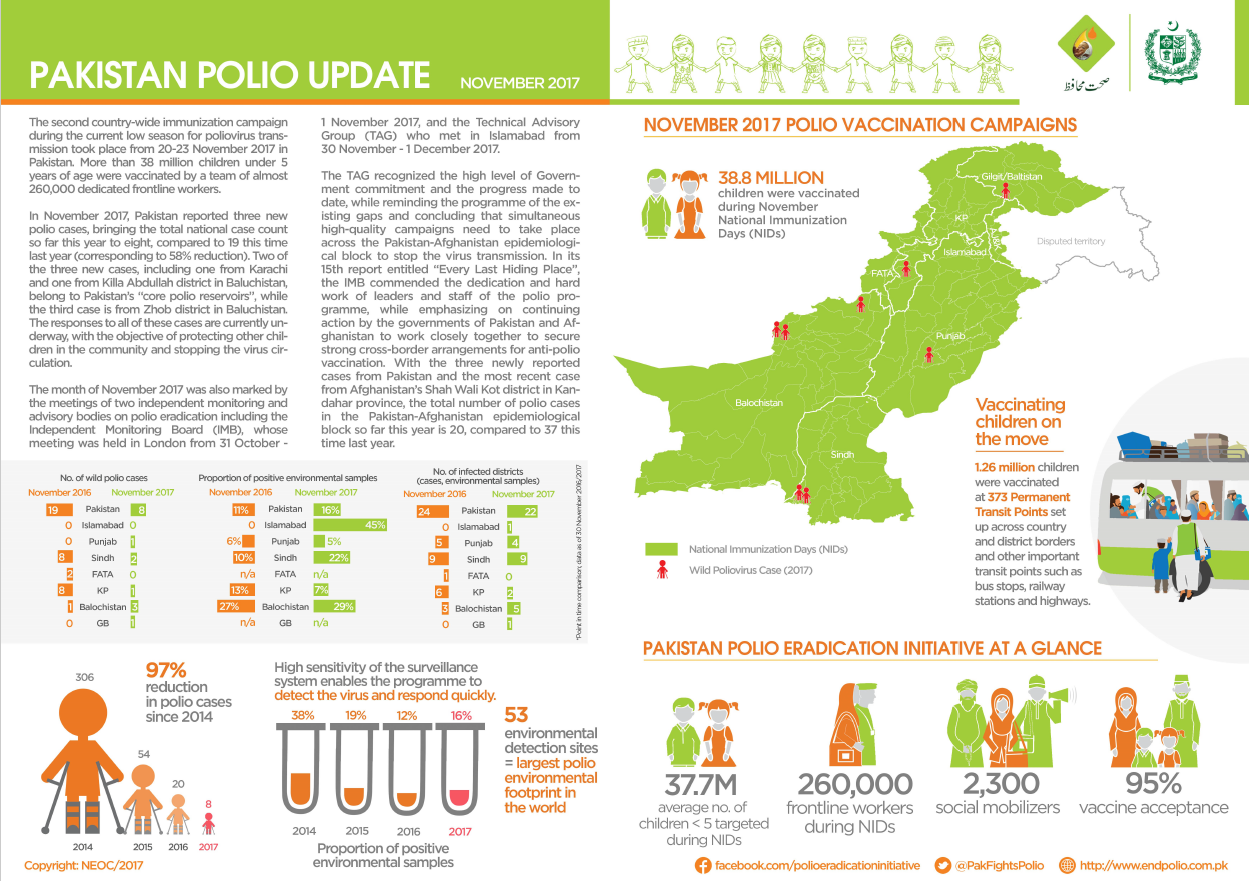
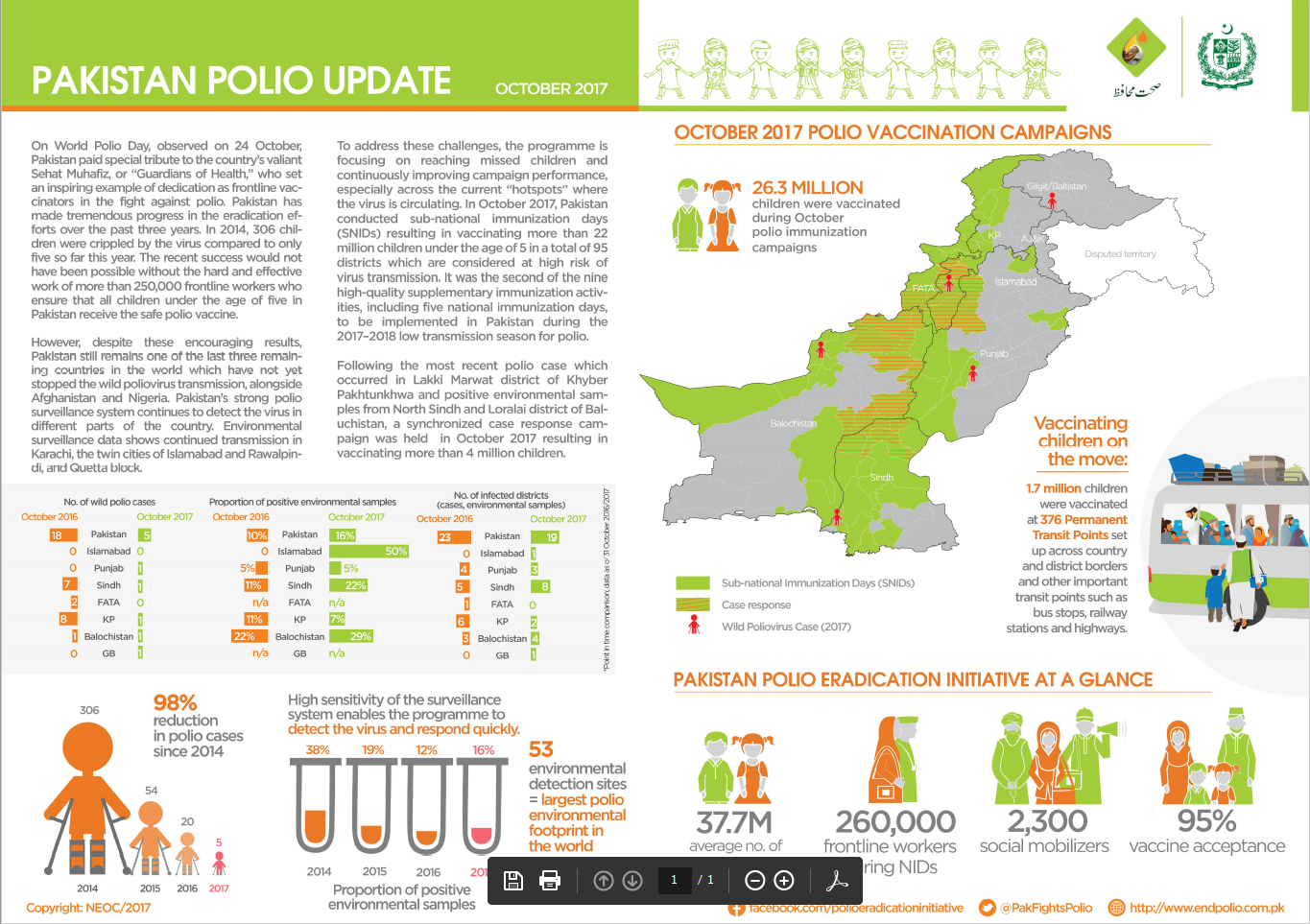
The Pakistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Pakistan.
October updates include:
No new cases of polio reported – the total for 2017 remains five.
Polio vaccination campaigns took place in priority areas of the country in October, successfully vaccinating around 22 million children.
Around 1.7 million children were vaccinated at 376 Permanent Transit Points set up across country and district borders, as well as at transit points such as bus stops, railway stations and highways.
On World Polio Day, observed on 24 October, Pakistan paid special tribute to the country’s valiant Sehat Muhafiz, or the “Guardians of Heath”, who set an inspiring example as dedicated frontline vaccinators in the fight against polio.
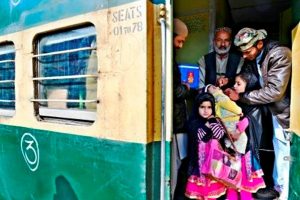
Dressed in a blue uniform, carrying a vaccine carrier on his shoulder, Imran Khan is a polio vaccinator working at Karachi Cantonment Railway station. “I make sure no child under five travelling by train is missed during the immunization campaign,” he says. Apart from vaccinating children, Imran also sensitizes their parents on the importance of vaccination and threats posed by the crippling disease.
Vaccinating children inside trains is a unique initiative introduced in Pakistan’s Sindh province which is connected with the rest of country through a railway network that transports millions of people every day. Passengers include people travelling to visit family and communities living on the border between Pakistan and Afghanistan as well as seasonal migrants and displaced populations. With many of these people moving between areas where polio continues to circulate, the threat of the virus continuing to survive as it moves from place to place via this human network is one of the biggest challenges the programme is facing. Reaching children on the move with the polio vaccine is therefore critical for stopping the virus.
Currently there are more than 500 permanent transit points across the country, where vaccination teams work to vaccinate all children under the age of five as they cross district, provincial and national borders. The strategy to vaccinate children inside trains themselves was started in Pakistan’s Sindh province in January 2017. Since then, during each vaccination campaign, polio workers vaccinate children travelling on the popular rail route between Karachi and Hyderabad, Sindh’s two biggest cities, which was selected for the project implementation.
“During campaign days, I travel from Karachi to Hyderabad on a daily basis. Along with other team members, we visit all the train compartments to vaccinate each and every eligible child”, says Imran Khan with passion in his voice.
According to Dr Nawab Khan, High Risk Mobile Population coordinator with Pakistan’s Polio Eradication Initiative: “To maintain and increase population immunity against polio in Pakistan, reaching children through public transport routes is an effective outreach strategy. It plays an important role in interrupting the transmission of poliovirus and represents a great opportunity to vaccinate children missed during door-to-door immunization campaigns.”
More than 24 thousand children have been vaccinated inside trains running between Karachi and Hyderabad since the project started.
It is thanks to the use of innovative strategies such as this one that the Pakistan Eradication Polio Programme has come so close towards achieving a future in which polio no longer endangers children, families, and communities. The progress can be seen in the declining number of wild poliovirus (WPV) cases in Pakistan: from 306 cases in 2014, to 54 in 2015, and 20 in 2016. As of October 2017, the total number of WPV cases reported in Pakistan stands at five.
Italy has provided €4.5 million to support efforts to reach and vaccinate all children under five years of age in Pakistan and Afghanistan – the only two countries worldwide that have reported polio cases this year.
In Afghanistan, the contribution will be used to support and train vaccinators and social mobilizers in generating demand for vaccination, the delivery of vaccines and monitoring whether vaccination activities are well-implemented. In Pakistan, the contribution will support vaccination campaigns in the most challenging areas of the country, as well as the immunization of communities that are at particularly high risk due to their mobility, through tactics such as giving vaccine established transit points.
The Bill & Melinda Gates Foundation have matched Italy’s contribution, doubling its impact to €9 million.
Polio is a highly infectious but entirely preventable disease which remains endemic in only three countries – Afghanistan, Pakistan and Nigeria. When the polio eradication effort was launched in 1988, there were 350,000 cases of polio every year across 125 polio-endemic countries. In 2017, there are 13 cases to date globally – 8 cases in Afghanistan and 5 in Pakistan, with Nigeria not recording any cases for more than 12 months.
This remarkable progress is thanks to the tireless work of committed front line health workers, governments and the five partners of the Global Polio Eradication Initiative: UNICEF, WHO, Rotary International, the US Centers for Disease Control and Prevention, and the Bill & Melinda Gates Foundation.
“The Italian Minister of Foreign Affairs, Angelino Alfano, underlined Italy’s commitment to a polio-free world for all future generations. “Italy is proud to support this immunization initiative which will not only rid the world of this devastating disease but improve children’s health and bring health returns and productivity gains for communities and countries’ economies,” Minister Alfano said.
UNICEF Director of Polio Eradication Akhil Iyer said that the funding would support efforts to generate community demand for vaccination and deliver vaccines in high-risk polio-endemic areas. “Italy’s contribution is critical in helping us to reach every last child in some of the world’s most challenging contexts, and to help us prove that we can live in a world where no child need be left behind,” Mr Iyer said.
WHO’s Director of Polio Eradication, Michel Zaffran, said new funding such as Italy’s was essential to ensure all children were covered during immunization campaigns. “As we reach the endgame of the polio eradication effort, the vaccination of what we call mobile populations – communities which are migrant or on the move – is essential to ensure all children are protected and the virus cannot spread from one area to another. This funding will directly help us reach and protect those most vulnerable populations,” Mr Zaffran said.
Malik is one of the hardworking vaccinators making sure that even children on the move are protected against polio.
The poliovirus knows no borders, making children on both sides of the border between Afghanistan and Pakistan vulnerable to contracting the debilitating disease. This is why, placed strategically along the border, 19 WHO-supported vaccination posts reach children on the move as they cross between countries, ensuring that all children under the age of 10 receive two drops of the oral polio vaccine to protect them from polio.
One of these teams is led by Malik, who has worked for the polio eradication programme for 14 years.
“I wanted to join the eradication programme when I heard that polio is a contagious disease that affects children. I wanted to serve children and our community. I learned about polio on the TV and radio and the health workers who came to our home to share information about the virus.”
Protecting children on the move
Malik started working as a vaccinator and has now worked as a team supervisor for the past 10 years.
“I am proud when we can reach every child and when I see my team vaccinating children, making sure that no child is missed. This makes me very happy,” he says.
Cross-border vaccination teams are crucial in the fight against polio. The Torkham border between Afghanistan and Pakistan, in eastern Nangarhar province, is one of the busiest border crossings in Afghanistan. Currently 38 WHO-supported vaccinators work in three shifts, operating 24 hours a day, 7 days a week.
“Today I started my work at 5.30 am. When we arrive at work in the morning, I gather the team together and we go through any issues that arose in the previous shift. We revise the schedule of the day and I assign teams to their specific locations. We have three locations at this border where we vaccinate all children coming to Afghanistan and those who are leaving.”
Since January 2017, WHO and partners have vaccinated over 44 000 Afghan children under the age of 10 crossing the border to Afghanistan from Iran and Pakistan. Over 25 000 of these have been vaccinated at the Torkham border’s so called “zero point” – the first point where Afghan refugees and returnees returning from Pakistan arrive.
“We focus a lot of finding cases of acute flaccid paralysis, sudden onset of floppiness in the limbs that is a sign of polio. We check children in all the vehicles that arrive at the border and work hard not to miss any potential polio cases,” Malik says. “When the trucks park here, we talk to the parents and ask about any possible cases of paralysis in the family. We also educate them about the importance of vaccines and tell them about the routine immunization services that are available free-of-charge in Afghanistan’s health facilities.”
Building trust
Most caregivers crossing the border to Afghanistan accept the polio vaccine but challenges remain.
“Sometimes we see parents who refuse to vaccinate children. We try our best to convince them to vaccinate by telling them more about the benefits of the polio vaccine and how polio cannot be cured. Those who refuse to vaccinate their children often don’t understand what the vaccine is or how it is essential for protecting their children,” Malik says.
Despite difficulties and his demanding work in a challenging environment where the security situation can shift quickly, Malik and his team are determined to continue the fight against polio.
“Afghanistan is still polio-endemic and the virus is deadly,” he says as he leads his team to approach another truck that crossed the border into Afghanistan. “I want to deliver these crucial services, serve my community and protect vulnerable children.
Rising up into the sky, a tower block’s outline trembles in the heat haze, even in the early morning. It’s hard to count the number of floors from the ground as the concrete block stretches up so high. Inside the door, you look around for an elevator – but there is none. Taking a deep breath and hoisting the vaccine carrier higher onto your shoulder, you begin the long climb up the stairs through the heat. At the top, many pauses for breath later, you knock on the first door. As a mother holding her baby opens it, your work for the day really begins – but there is a long way to go. To vaccinate every child in the city against polio, you and your fellow vaccinators must knock on every door in this building; on this street; in this neighbourhood; and across the entire city. It is a monumental task – and one you take on several times a year.
Cities: Uniquely challenging environments
Often it is the ability of polio vaccinators to reach the most remote and inaccessible villages, hampered by challenging weather or conflict, that is the biggest challenge to eradication. But big cities, while more easily accessible, can pose an equal challenge.
Dr Mohammed Sibak Abouzeid, has been working to stop polio in Egypt since 1999, planning and organising polio eradication campaigns and evaluating whether enough children were reached in each campaign so that the next one can be better. Over 40% of Egypt’s population lives in urban environments.
“While my colleagues in the countryside are battling challenging terrain, weather and long journeys, we have a different set of barriers: slums, high rise buildings, marginalised communities and big populations that can change overnight,” says Dr Mohammed. “But our goal is the same: to reach every single child, no matter where they live.”
One critical tactical shift to ensure all floors of a tower block were covered was to ensure vaccinators first walked to the top floor, and then knocked on every door coming down, rather than the other way around, which meant the very top floors were missed.
A playground for polio
Cities provide an easy environment in which for polio to spread. The poliovirus spreads between humans through faeces, so wherever sanitation systems or hygiene practices are poor, or many people live in close quarters, the virus is able to spread rapidly.
Vaccination teams go door to door in urban slums such as this. This location is also used to collect sewage water which is tested for poliovirus as part of the country’s environmental surveillance network. UNICEF/S. Biswas
The city of Karachi is one of the remaining strongholds of the virus. People move in and out of Pakistan’s biggest city constantly: these ever changing populations make it difficult to know how many children need to be vaccinated and where they live. Many children are born every day, giving the virus many opportunities to hide in the unvaccinated guts of infants who have not received at least three doses of polio vaccine. Given the informal nature of many of the slums within this city, the lack of infrastructure such as health care centres can make it especially difficult to get vaccines to every child.
Slums have another consequence for polio eradication; with high levels of poverty, malnutrition and diarrhoea are regular threats. Malnutrition can damage the immune systems of children, meaning that even if they receive the vaccine, it might not be able to kick start the process of generating protection against the virus. Diarrhoea can lead to the vaccine leaving the body too quickly for it to begin creating antibodies; but it also can act as a vehicle to cause the poliovirus to spread further and faster.
Stopping polio in cities
Stopping polio even in these challenging environments takes ingenuity and creativity. Luckily, people like Dr Mohammed have the experience necessary to make a difference.
“To stop polio in urban environments, you need to train all vaccinators incredibly well, and give them the motivation they need to work in difficult environments. But the most important thing is to come to understand the networks that city inhabitants are a part of so that you can engage them, involve them in vaccination campaigns and find the right influencers from local communities to encourage parents to vaccinate their children.”
In cities like Cairo in Egypt and Mumbai in India, once thought to be the hardest places in the world to stop polio, such tactics were instrumental in stopping poliovirus. Indeed, they continue to be used even now in order to ensure high vaccination coverage and keep their populations protected. It may be a matter of getting the right neighbourhood religious leader to announce vaccination campaigns during a sermon, or the right midwife to tell new mothers about vaccination, but one thing is for sure: success against polio is ensured one person at a time, even in a city of millions.
Read more in the Reaching the Hard to Reach series
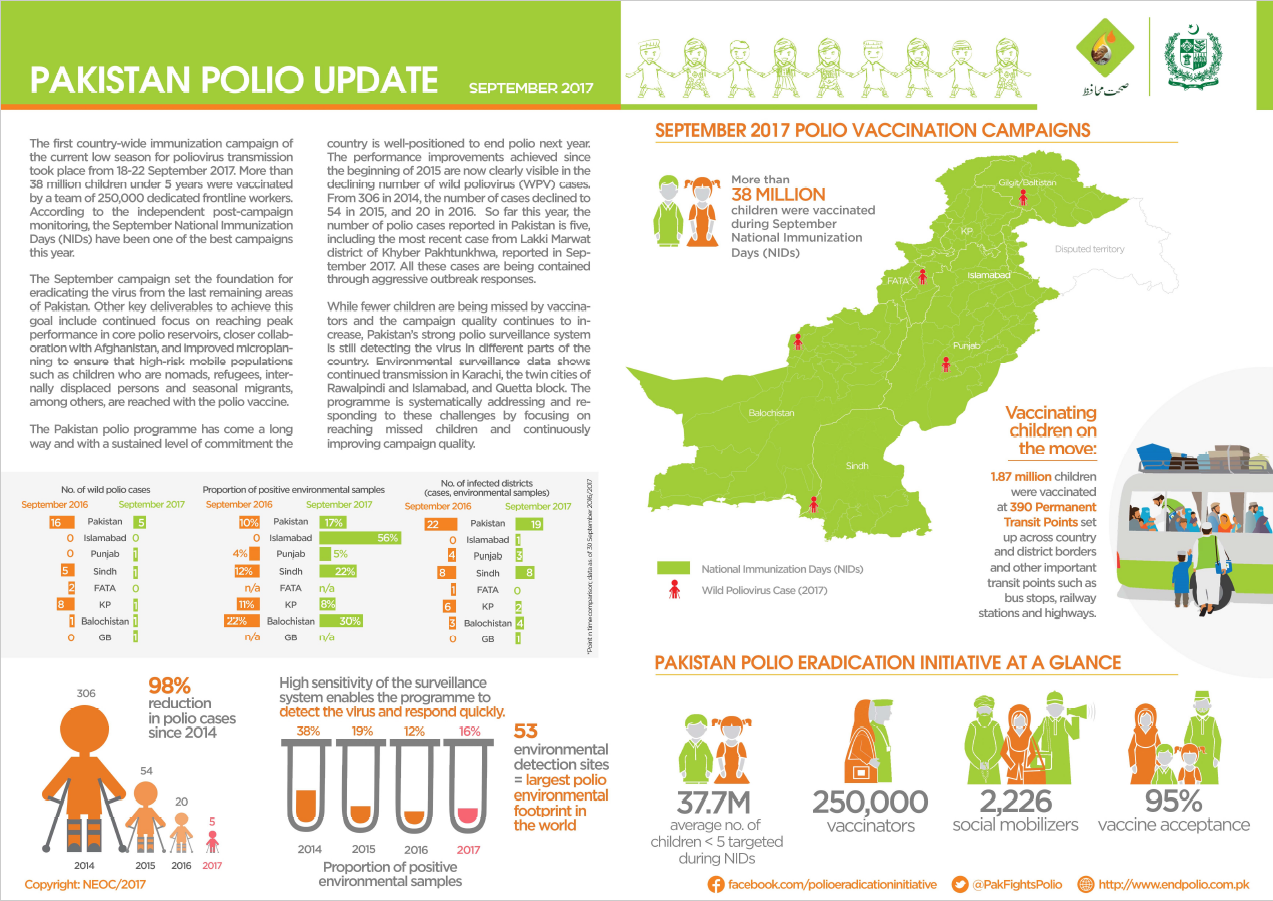
The Pakistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Pakistan.
September updates include:
No new cases of polio reported since the August update – the total for 2017 is five
The first country-wide immunization campaign of the current low season for poliovirus transmission took place – 38 million children under 5 years were vaccinated.
According to independent post-campaign monitoring, the September National Immunization Days has been one of the best campaigns this year.
The September campaign set the foundation for eradicating the virus from the last remaining areas of Pakistan.
It’s a clear, summer day in Safdarabad, in the Punjabi province of Pakistan, and Mr. Patras Maseeh Bhatti and his colleagues have just arrived at “work” for the day. Surrounded by brick buildings instead of the inside of laboratory, they might look out of place in their attire. Dressed from head to toe in bio-hazard lab coats, long black rubber boots, and thick industrial gloves and armed with a bucket, their mission is to collect enough sewage from the selected sample site to be transferred in a separate container to the laboratory in Islamabad. Once there, the sample will be tested for poliovirus.
This sampling is part of a system of disease surveillance, which underpins the entire global effort to eradicate poliovirus. Without surveillance, it would be impossible to pinpoint where and how wild poliovirus is still circulating, or to verify when the virus has been extinguished from the wild.
Across the Eastern Mediterranean Region, disease detectives like Mr. Bhatti are becoming more and more important in the fight to end polio. In addition to surveillance for Acute Flaccid Paralysis (AFP), which involves the detection and reporting of children with rapid-onset ‘floppy’ limbs, environmental surveillance involves testing sewage or other environmental samples for the presence of poliovirus.
“This is the only mechanism where you will be able to detect viruses that are circulating with the absence of paralytic polio cases,” Dr Humayun Asghar of WHO’s Regional Polio Programme explains. “As we get closer to eradicating polio even with very high [vaccination] coverage in the population, the virus can still circulate undetected in under-immunized children.”
The growing network of disease detectives
Although AFP surveillance remains the gold standard for surveillance for polio, only one in approximately 200 cases of polio actually show symptoms of paralysis. The World Health Organization has been working closely with a number of countries within the Eastern Mediterranean Region to expand environmental surveillance networks and build capacity in field and lab staff. In endemic areas, environmental surveillance is providing critical supplemental information and data, enabling epidemiologists to tailor the eradication strategies even further. In other parts of the Region, it is proving a critical additional tool to mitigate the risks of a potential virus importation, particularly given the challenges that some countries face, including large-scale population movements, inaccessibility or insecurity.
“In these situations, any additional tools to supplement our AFP surveillance are critically valuable,” he says, “and we need a robust system in place for countries to be able to manage this network.”
In countries like Pakistan and Afghanistan, Dr Asghar says rapid and extensive population movement is the biggest risk for the virus spreading. “The virus moves with the people, so we cannot be sure that the virus is staying where we detect the cases. Here, environmental surveillance has proven extremely valuable because in the absence of many paralytic cases, we continue to detect wild poliovirus in the environment which tells us a lot about how and where the virus might be continuing to hide.”
The detection of poliovirus in countries not recording paralytic cases is also very useful, Dr Humayun says. During the polio outbreak in the Middle East in 2013-2014 this helped to inform partners carrying out the multi-country regional response where to further concentrate efforts in order to close the outbreak and ensure it did not spread further.
In both Pakistan and Afghanistan, environmental surveillance has been one of the key strategies for narrowing in on where the virus continues to circulate, and the lessons learned through the establishment of environmental surveillance in these countries is informing the expansion across the region.
In Lebanon and Jordan, where environmental sampling has been established in 2017, staff have been trained to collect samples from specified collection sites and to ensure the samples reach the laboratory in Amman in the right condition for processing.
Efforts to build on existing health infrastructure and disease surveillance systems in Iran, Sudan, Somalia, Syria and Iraq are underway, with plans for the expansion of environmental surveillance systems and lab networks in 2017.
Leaving a lasting legacy for health systems
Since the Global Polio Eradication Initiative (GPEI) began in 1988, the programme has mobilized and trained millions of community health workers and volunteers for surveillance. A standardized, real-time global surveillance and response network exists and is being put to full use.
Dr Humayun says that this investment in people and infrastructure is not only of benefit during the last mile of polio eradication, but will be a lasting legacy that the polio programme will leave behind for health systems of countries across the region.
“Polio surveillance methods, techniques, facilities and knowledge are our biggest assets, but they have applications beyond our programme. So, these laboratories can be of great value then to countries who need to develop their capacity in other diseases of public health importance,” he says.
The Pakistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Pakistan.
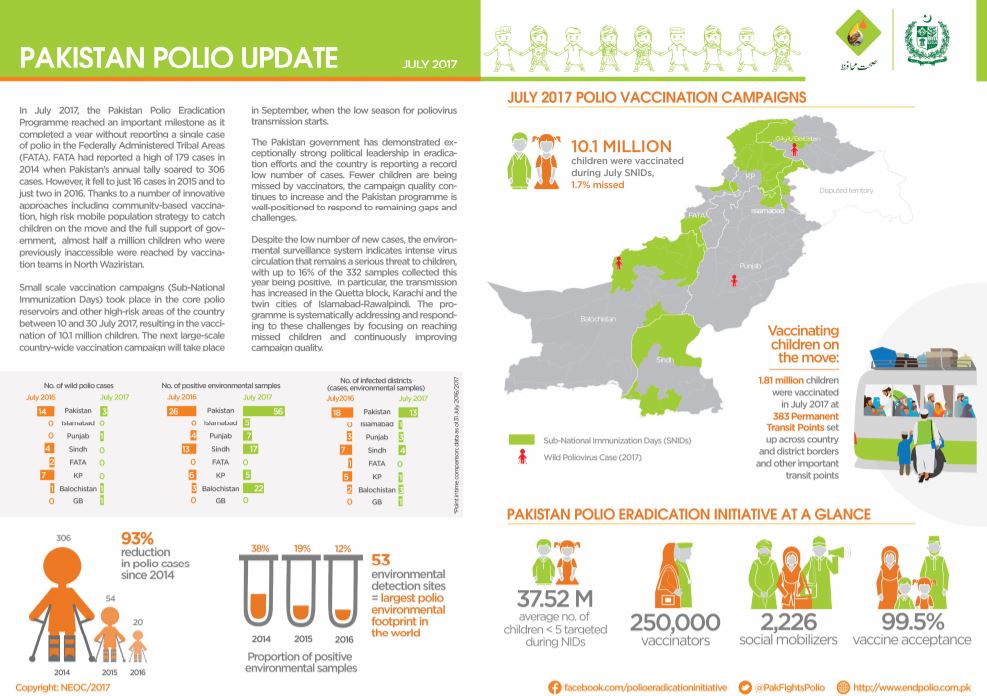
July updates include:
No new cases of polio reported – the total for 2017 remains 3
The Federally Administered Tribal Areas marked one year without reporting a case – down from a high of 179 cases in 2014
Small-scale vaccination campaigns were carried out in July in the core polio reservoirs and other high risk areas, aiming to reach 10.1 million children
Fifty-seven year-old Khalida, a striking figure on her four-wheeler motorbike, is a supervisor of one of the female vaccinators’ teams in Karachi, Pakistan’s largest city.
“I have been working as a supervisor for three years, but I have been associated with polio vaccination campaigns for many years as volunteer,” she explains. The community in the area where Khalida works is mostly from Pakistan’s tribal areas in the north-west of the country, and distrustful of outsiders. Traditionally, this mistrust involved not accepting vaccination. Today, all families in the area accept polio drops.
Khalida had worked in different jobs but wasn’t satisfied until she was offered a job of polio team supervisor. Her influence in the area has been critical to overcome myths about vaccination and build knowledge and trust.
Having women like Khalida working on the frontlines is a game changer for polio eradication. The fact that she is well known and trusted in her community means that mothers and fathers are more likely to allow her and her team to take the crucial step across the thresholds of their homes to vaccinate their children. The Pakistan Polio Programme’s emphasis on local, motivated, full-time, community-based female vaccinators has been improving immunization coverage figures. Across the country, the proportion of vaccinated children increased from 85% in August 2016 to 92% in May 2017, according to independent post-campaign monitoring.
In my community, the number of polio cases has decreased drastically. The progress is visible with the naked eye. We hold rigorous polio campaigns which are being carried out frequently in the area to reach every child multiple times with vaccines and keep them safe against paralysis. In this regard the contribution of the frontline health workers I supervise is remarkable, as they work hard to ensure each and every child is protected from this crippling disease.
Polio eradication is very important to have a healthy generation; as healthy generations, these children will be able to better serve the country – Khalida
For Khalida, vaccinating children against polio is a true mission. “Since I began working to end polio, I feel like I am a soldier. Just as an army fights to protect a country, similarly I fight against a virus which is disabling our beloved children. I will fight against this crippling disease until the virus is permanently eradicated and our beloved children are fully protected”.Khalida’s work spans a large area, with temperatures in the summer reaching 40°C, making the work of vaccinators very challenging. To provide supervision to the polio teams under her care, Khalida uses a motorbike specially designed for her for this very purpose – it has four wheels and is capable of crossing the rocky terrain and getting her where she needs to go at top speed. The sight of Khalida coming into a settlement on her motorbike has become a well-known, welcome sight.
Pakistan is one of only three last polio endemic countries, along with Afghanistan and Nigeria. The number of cases has declined dramatically in the past years: from 306 in 2014 to 20 in 2016. As of June 2017, the number of polio cases reported in Pakistan was three.
A child receives two drops of polio vaccine during the May vaccination campaigns in Lahore, Pakistan. WHO Pakistan/Anam Khan.
At the end of May 2017, more than 38 million children under the age of 5 were vaccinated against polio in Pakistan. During the campaign, over 250,000 trained polio workers went from house to house across the length and breadth of the country to vaccinate children against the crippling disease.
This was one of five country-wide vaccination campaigns that took place during the 2016/2017 “low season” for poliovirus transmission. From October to May when temperatures are low in Pakistan, the virus remains less active, giving polio eradication experts the opportunity to get ahead of the virus.
The end of the May polio campaign marked the start of the “high season” for poliovirus transmission. The ability of the poliovirus to infect children increases in high temperature and during heavy rainfall. As a result, viral circulation is expected to be higher from June to September.
Reaching more children
With steady gains in the proportion of children vaccinated during the 2016/2017 low season, the May campaign achieved an overall goal of vaccinating 92% of the targeted children, according to independent post-campaign monitoring. The highest vaccination coverage rates were observed in Khyber Pakhtunkhwa (KP), Sindh and the Federally Administered Tribal Areas (FATA), some of the highest risk areas of the country, with rates increasing from 84% to 95% in KP and 77% to 93% in Sindh in the last nine months.
A polio vaccinator marks the door of a house to show that the children living there were not home when he called, so that they can be vaccinated by campaign monitors the next day. WHO Pakistan /Anam Khan.
However, more work is needed to bring vaccination rates up to 95%, the level identified as that needed to stamp out the virus for good. FATA remains the only region consistently over 95% in the last three campaigns, with Balochistan, Islamabad, Azad Jammu, Kashmir and Gilgit Baltistan not reaching the benchmark.
With the high season underway, Pakistan is well-positioned to respond to these remaining gaps and challenges. The current situation remains the best we have ever seen in the country, with the virus geographically limited. The number of cases has declined from 306 in 2014 to 53 in 2015, and to 20 in 2016. So far this year, the number of polio cases reported in Pakistan is three (compared to 13 the same time last year). However, this progress means that there is more to lose than ever before. The low season campaigns put the polio programme in a better position with which to fight the virus through the high season.
Poliovirus in the environment
While the number of new wild poliovirus cases remains record low, the environmental surveillance system indicates the virus remains a serious threat to children, with the proportion of samples being tested positive for poliovirus reaching 18 per cent as of May this year compared to 10 per cent as of May 2016. In particular, the environmental presence of the virus has increased in the Quetta block, Karachi and the twin cities of Islamabad-Rawalpindi. The programme is systematically addressing and responding to these challenges by focusing on reaching missed children and continuously improving campaign quality to remove every last hiding place of the virus.
A father and daughter proudly show off the purple dot of ink on her little finger to show that she has been vaccinated against polio in the May campaign. WHO Pakistan/Anam Khan.
Preparing for the next low season
Government leadership is fully committed to the National Emergency Action Plan (NEAP), implemented via focused Emergency Operations Centers at National and Provincial levels, with emphasis on evidence-based decision making, a one-team approach between all of the partners of the GPEI and the government, highlighting the essential role of front-line workers at the center of the polio eradication effort, effective oversight of performance management and accountability, and coordination across the common Afghanistan-Pakistan epidemiological block. As eradication moves into the final stage, seamless cross-border coordination with Afghanistan, that has had four polio cases so far this year, becomes ever more critical to success in both countries.
A US$ 33.3 million grant from the Government of Japan in humanitarian emergency funding to UNICEF was announced this week and will help to protect millions of children from polio in Nigeria and the Lake Chad region.
In response to the urgent need to rapidly raise immunity to polio virus in the region, Japan has generously provided exceptional funding from their supplementary budget envelope to purchase polio vaccines, conduct house-to-house polio campaigns and support communication efforts to mobilize communities for vaccination in Nigeria, Chad, Niger, Cameroon and the Central African Republic.
The detection of wild poliovirus in north-eastern Nigeria occurred in August 2016 following the large-scale movement of families affected by conflict in Borno State out of areas inaccessible to health services. National Governments, in collaboration with the Global Polio Eradication Initiative (GPEI), comprising the World Health Organization, UNICEF, Rotary International, CDC and the Bill & Melinda Gates Foundation (BMGF), have implemented emergency vaccination campaigns throughout the region to rapidly raise childhood immunity to the polio virus and guard against further spread.
UNICEF Director of Polio Eradication Mr Reza Hossaini said the Japanese funding was gratefully received and filled an urgent need. “This additional funding is very timely to support the ongoing polio vaccination campaigns and give Africa the very real opportunity to be completely polio-free,” Mr Hossaini said. “These campaigns aim to not only stop transmission of polio in north-eastern Nigeria but protect its neighbours against the spread of the virus through provision of vaccines and targeted social mobilization activities.”
Japan remains one of the champion donors to the GPEI and the Global Health agenda in general, with contributions to polio eradication through UNICEF since 2002 totalling more than US$ 333 million. This funding – and the leadership provided by both the Tokyo International Conference on African Development (TICAD) process and the Japan International Cooperation Agency (JICA)’s innovative soft loan in partnership with BMGF in Nigeria and Pakistan for polio eradication – has proven instrumental in the historic reduction of wild poliovirus transmission globally.
In 2016, wild poliovirus transmission was limited to just 37 cases globally in the three remaining polio-endemic countries – Nigeria, Pakistan and Afghanistan. This year, to date, only two cases have been recorded worldwide, in Afghanistan. However, while the opportunity to finally eradicate polio is real, the risk remains: as long as one child is infected, every child remains at risk. It is critical that all countries continue to maintain high immunity to polio until the virus is eradicated, once and for all.
The border between Pakistan and Afghanistan is no barrier to the poliovirus. Close cultural and linguistic ties connect the two countries. Populations move fluidly across these borders. Each year, the virus moves with them.
Afghanistan and Pakistan have seen significant progress in the last 18 months in their efforts to stop polio. But both countries have been close before, and have been thwarted: the virus has found pockets of unvaccinated children where it can hide, regroup, and stage a comeback. Despite historically low levels of polio over the last few months, cases of paralysis and positive samples found through environmental surveillance show us that the virus has not yet been stopped.
A new approach
Armed with this knowledge, Pakistan and Afghanistan have taken a new approach. Since June 2015, the two have been coordinating major programme activities, as success in one country depends on success in the other. Monthly polio immunization campaigns have been synchronized so that no child on either side of the border can fall through the cracks, the Emergency Operations Centres (EOCs) of each country – which house the government and partners of the Global Polio Eradication Initiative to coordinate eradication activities – interact with one another on a weekly basis, and the highest level political and administrative leadership meet face to face every six months, to resolve challenges and to develop plans to address the remaining hurdles.
A common communications strategy has synchronized messaging at the border and – with radio being the main source of news for 70% of Afghans and 50% of Pakistanis in border areas – the programme has coordinated radio programming on the leading border channels, producing weekly health shows and using popular soap operas to create Pashto-language programming on polio and children’s health.
This innovative approach is paying dividends. The polio eradication programmes in both countries are working closely together to coordinate vaccination campaigns, surveillance, and to track population movements.
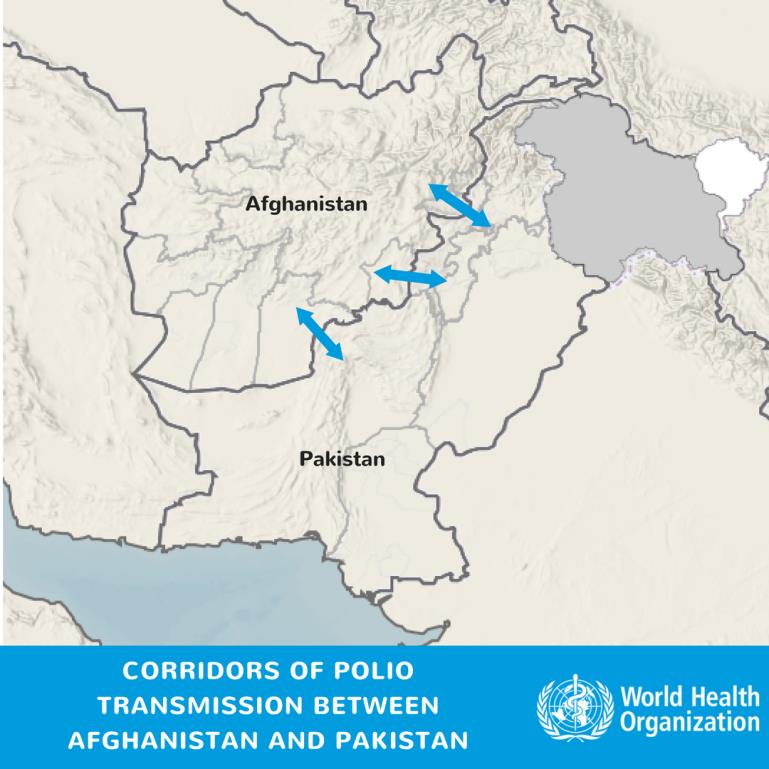
The three ‘corridors’ of polio transmission
Three ‘corridors’ are serving to allow the virus to travel with population movements between countries: via the Torkham border crossing from Peshawar and Khyber in Pakistan to Nangarhar, Kunar and Laghman in east Afghanistan, and via the Friendship Gate border crossing from Pakistan’s Quetta Block to the Greater Kandahar area in south Afghanistan. Population immunity in these transmission corridors have been gradually improving in the last year, shown by the vaccination status of non-polio AFP cases.
Wild polio increasingly seems to be travelling down a central corridor between southern Khyber Pakhtunkhwa and the Federally Administered Tribal Areas in Pakistan travelling across rugged, smaller border crossings to Paktika, Paktia and Khost provinces in the south east of Afghanistan.
Mobile populations
At the most recent Inter-Country Coordination Meeting in Islamabad, Pakistan, the Afghanistan National EOC Director underscored the importance of reaching and vaccinating populations on the move, whether at formal or informal locations.
While Torkham in the northwest and Friendship Gate in the south are the main border crossing points between the reservoirs – with more than one million children under 5 crossing these points each year – the smaller informal crossings are considerably more challenging to reach and vaccinate children.
Pakistan and Afghanistan are working to strengthen coordination on the communities moving through these locations, to ensure that all children under 5 are vaccinated wherever they are. The programmes are strengthening their disease surveillance at community level, mapping out mobile groups and ensuring they’re included in immunization microplans, and working with leaders and influential figures to understand their movements better.
Stronger together
The new polio cases in the central corridor have reinforced the idea that neither Pakistan nor Afghanistan can eradicate polio alone, with the virus travelling between the two. At the Islamabad meeting, the National EOC coordinator for Pakistan highlighted the fact that neither programme was where it intended to be by this time in 2016, and these strategies tailored to addressing specific challenges were essential to end the virus for good.
The significant improvements in the programme quality in the southern and eastern corridors can be attributed to a relentless focus on improving campaign quality and the innovative approach of the two countries working as one team across the border.
Pakistan and Afghanistan are learning from the programme’s experiences in other countries. If this progress can be maintained in the traditional corridors between the long-time polio reservoirs, and the programme can move quickly to rapidly increase immunity in the new, central corridor, the programme has the opportunity to strike out polio in two countries with one blow, working together to ensure that no poliovirus can find a hiding place along the porous border between them.
The Global Polio Eradication Initiative (GPEI) is highlighting the innovations that are helping to bring us closer to a polio-free world. Find out about other new approaches driving the polio eradication efforts by reading more in theInnovation Series.
In the last stages of polio eradication, a sensitive surveillance system that can detect every single poliovirus is indispensable to find it in its last hiding places. In Pakistan, surveillance for cases of acute flaccid paralysis (AFP), subsequent testing and supplementary environmental sampling from the environment are informing the progress made towards eradication.
The poliovirus has proven to be a constant and resilient foe, continuing to show up in several areas of Pakistan. However, transmission is the lowest it has ever been. So far in 2016, fewer children have been paralysed by polio than at any other year in history, with the virus limited to a few areas in just three countries – Pakistan, Afghanistan and Nigeria. Pakistan has made strong progress in identifying and vaccinating missed children in the country’s most challenging areas, resulting in historical low numbers of cases this year. This remarkable achievement is especially visible in the core reservoir districts where persistent transmission has been the norm.
Training surveillance officers
The training of dedicated surveillance officers is key to ensuring Pakistan’s surveillance system is built strongly for eradication. A recent training for 32 district surveillance officers from across Pakistan highlighted the importance of effective AFP and environmental surveillance in tracking down the virus. World Health Organization’s National Surveillance Coordinator, Dr Tahir Malik said the training is essential to ensure surveillance officers down to the district level are highly skilled in identifying and investigating cases. “This is critical not only to orient new surveillance officers but also for old officers to bring alignment in surveillance procedures”. He further explained, “After training we expect from the participants to fully understand poliovirus epidemiology, AFP surveillance, but also in detail its components and mechanics in Pakistan.”
“The training, which also covered specifics on the role of laboratory, surveillance indicators, healthy children sampling and environmental surveillance, aims to bring all officers on one page in terms of programme priorities,” Dr Tahir said.
Constantly improving
Supported by contributions from the Canadian Government, the training is part of the programmes surveillance improvement plan that was recommended by the Technical Advisory Group (TAG) for Polio Eradication in Pakistan, to place a greater emphasis on disease surveillance including scaling up the workforce of dedicated staff, realigning environmental surveillance sites and ensuring surveillance targets are met by including private and informal health sectors, pushing for timely investigation, and reprioritizing reporting sites to focus on silent UCs and Tehsils.
The Chairman of the TAG Jean-Marc Olive, who was visiting Pakistan during the training, addressed the Surveillance officers from Punjab, Balochistan, FATA and KP. “Make the paediatrician your friend, talk continuously to the community, walk, move, sensitise, orient, visit facilities and care providers. Surveillance is not beautiful graphs on a laptop, it is hard field work,” he said. “Be proud of what you do for the children of Pakistan.”
The 2016-2017 National Emergency Action Plan for polio eradication also highlights the intensification of surveillance as a critical activity so that virus signal are picked up as early as possible and response initiated rapidly and aggressively. In response, the programme is working to engage private clinics, traditional healers and pharmacies to make it more likely that all cases of polio will be reported and immediate case response can be launched when needed.
Environmental surveillance
In addition, there has been an increase in the work being done for environmental surveillance. The number of sites that test for presence of the virus in sewage water has been increased to 43 sites across Pakistan’s highest risk areas and environmental samples are being taken more frequently, which is proving to support the programme to detect and track the virus, a critical step as the country edges closer to stopping transmission.
Leaving no stone unturned
Once Pakistan is able to demonstrate that no poliovirus is present, both from AFP surveillance and supplementary environmental surveillance, for three consecutive years, the country will be declared polio-free. Until that time Pakistan will continue to leave no stone unturned in pursuit of the virus and no child unvaccinated and vulnerable.
Canada is one of the leading supporters of the Global Polio Eradication Initiative’s goal of eradicating the disease by 2018, and this year again extended its support to polio eradication in Pakistan with a renewed commitment of Can$40 million. The contribution, in part made through WHO, continues to contribute to the efforts to strengthen the monitoring and surveillance of the virus to track it down to its last hiding place.
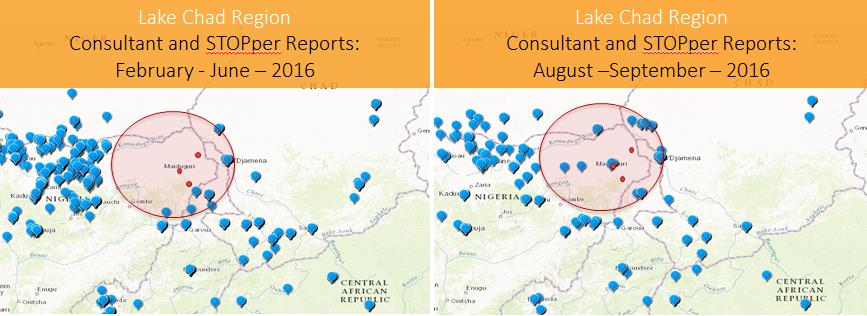
The polio eradication programme is using technology in innovative ways to map the activities of polio workers on the ground, and ensure that expertise and support is getting to the areas where it is most needed.
More than 300 international consultants are deployed by the partners of the GPEI in some of the countries most vulnerable to polio. By strengthening surveillance, tracking the virus, identifying immunity gaps and supporting vaccination campaigns to fill them, these consultants provide an important boost to capacity in polio-affected or vulnerable countries. By using new technologies, the programme is mapping the activities of all consultants to capture the range of locations they travel to and the activities they carry out. These innovations ensure that countries receive the best support from these consultants, and that they are working where the need is greatest.
Survey 123
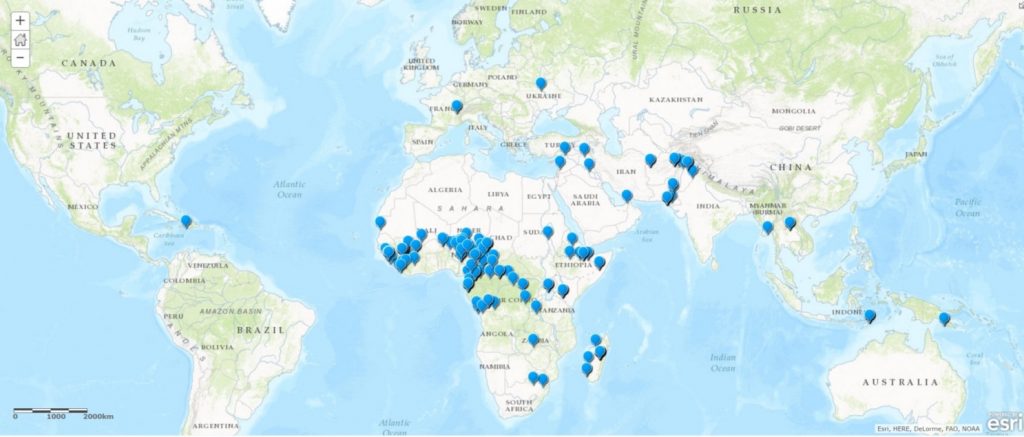
The introduction of this new technology means that each week, no matter where they are in the world, international consultants report on their activities using a smartphone application called Survey123. The report only takes a minute to complete, works offline and captures their location at the time of reporting. By answering questions on what activities and diseases they have been working on that week, this tool enables the GPEI to capture data in real-time and ensure international consultants are being efficiently deployed in high risk polio areas and being used to their greatest advantage.
In the below snapshot from the first week of October, reports from the consultants can be seen in Guinea, the Lake Chad region, Madagascar, Somalia, Afghanistan and Pakistan – the areas that are most vulnerable to the virus.
From the 3 – 9 October, 242 out of 300 users completed an activity report using Survey 123, giving the programme essential information about their location and activities. Over 5000 reports were captured between February and September.
Getting people where they are most needed
Survey123 is also enabling the GPEI to identify changes in deployment over time. The recent notification of wild poliovirus in the Lake Chad region demonstrated the use of this clarity, by showing the movement of consultants into and around the Lake Chad region, despite insecurity and inaccessibility.
In depth analysis such as this provides greater clarity on what additional human resources are needed to respond to outbreaks or newly recognised risk areas, and indicates how rapidly GPEI resources can be used to fill important needs.
Following cases of polio being found in Nigeria in July 2016, Survey 123 was able to show the movement of international consultants into the affected areas to strengthen the response effort.
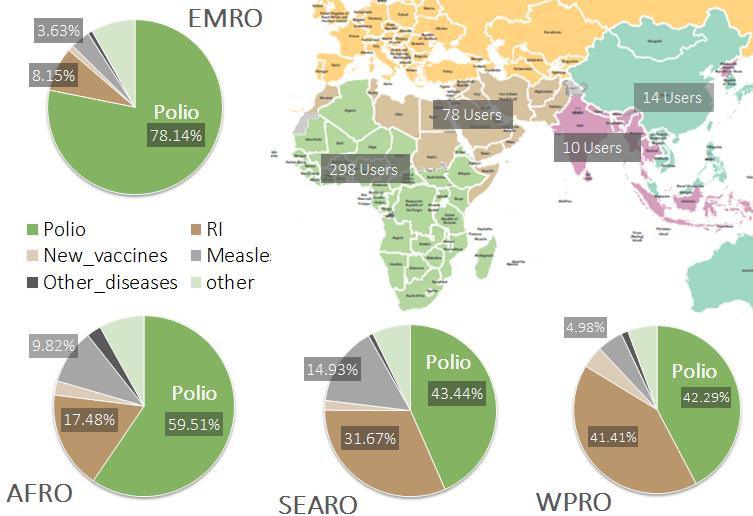
The broader benefits of polio eradication
Due to the scale of polio eradication activities even in the most remote and vulnerable areas to reach every last child, international consultants are sometimes present where other health infrastructure is weak. The capacity of the polio programme in these vulnerable areas is sometimes used to support other health initiatives, including improving routine immunisation, measles activities, communication for development and emergency response.
Analysing the collected reports from Survey 123 is giving us greater insight into the extent to which consultants are supporting other health programmes. The support provided to other health programmes shown in the map below highlights the continued benefits of the polio eradication infrastructure to other public health initiatives, giving the donors to the GPEI more bang for their buck when investing in polio eradication. The information gathered from this new technology is helping to inform transition planning efforts, providing information needed to country governments and GPEI partners as they look ahead to what should happen to the polio eradication infrastructure once the goal of a polio-free world has been achieved.
International consultants working on polio are also helping to support other health programmes. This map shows the amount of time in the different WHO Regions being spent on both polio and non-polio activities.
The Global Polio Eradication Initiative (GPEI) is highlighting the innovations that are helping to bring us closer to a polio-free world. Find out about other new approaches driving the polio eradication efforts by reading more in the Innovation Series.
The Regional Director of the World Health Organization speaks to the Technical Advisory Group on polio eradication efforts in Islamabad. – WHO/E.Sykes
The Technical Advisory Group (TAG) on polio eradication has met in Islamabad for the second time this year to discuss progress, remaining obstacles and opportunities as Pakistan edges closer to achieving the goal of stopping transmission of the virus.
Senior leaders from across the Global Polio Eradication Initiative joined Federal and Provincial team leads as they briefed TAG members on the progress made since the last meeting in January 2016. The group also assessed plans for updates to the 2016/17 National Emergency Action Plan leading into the next low transmission season.
Progress in Pakistan
As of the end of June 2016, 12 cases of wild poliovirus type 1 have been reported, a 57 per cent reduction from the same time in 2015. This improvement was attributed by the Global Polio Eradication Initiative to the united front now being presented by the team of partners working together under the leadership of the government through a network of Emergency Operation Centers. Progress was also ascribed to other strategies, such as the expansion of community based vaccination and health camps, which have helped with enhancing community ownership of the programme interventions. In addition, thousands of trained and dedicated frontline workers have ensured that 280 million children have received polio drops during nine campaigns conducted in the low transmission season. The successful campaigns of the inactivated polio vaccine in targeted high risk areas of Karachi, Khyber Peshawar and Quetta block helped in quick immunity boosting of approximately 3 million vulnerable children.
“The Government of Pakistan will remain committed to achieving our collective goal of polio eradication and thanks all our partners for their technical, financial and political support as we approach a significant milestone in global health,” said the Prime Minister’s Focal Person for Polio Eradication, Senator Ayesha Raza Farooq at the TAG meeting.
Overcoming the remaining challenges
The National Coordinator of Emergency Operations Centre, Dr Rana Safdar, outlined the overriding priorities for the National Emergency Action Plan for 2016-2017 as to ensure all children are vaccinated especially the most young in our most high risk districts; the detection of every signal of the polio virus and any emerging immunity or performance gaps; and to respond rapidly, aggressively and comprehensively to every significant event with implications for interruption of the wild polio virus.
The TAG recommended that efforts continue to be made to strengthen community based vaccination and mobile team performance, to reach every last child in all districts. They highlighted that stopping transmission in North Sindh was of utmost importance. Recommendations were also made to strengthen surveillance, to coordinate with Afghanistan along border areas and to strengthen routine immunization through the community based vaccination initiative.
The TAG also voiced appreciation for the progress made by in Pakistan over the past six months and urged the programme to maintain the quality of campaigns by focussing on improving the overall performance and decreasing the number of missed children in the core reservoir areas, and to identify and address the residual risks and to act swiftly in response.
World Health Organization’s (WHO) World Immunization Week 2016 kicks off this week with the aim of raising international awareness on the critical importance of full immunization from childhood through to adulthood. One of the campaign’s major focuses is the crippling poliovirus; incurable, but preventable with a simple vaccine. World Immunization Week is an opportunity to celebrate the progress marked by the drop in cases by 99.9% in the last three decades; but it also calls for increased momentum for the final push to overcome the last remaining pockets of the virus and wipe out the disease.
This World Immunization Week, experts are cautiously optimistic that we could see the end of the virus very soon. In 2015, a total of 74 cases of polio were reported in Afghanistan and Pakistan, the only two remaining polio endemic countries, down from 334 cases worldwide in 2014.
“We’ve come a long way since the establishment of the GPEI in 1988, from 125 polio-endemic countries to just two,” said Chris Maher, manager of WHO’s regional polio eradication unit in Amman, Jordan. “We are at the final frontier of eradication. A lot of work is still needed, but if we can stop polio transmission in Afghanistan and Pakistan by the close of 2016, the whole world will finally be free of wild poliovirus.”
As pressure mounts around achieving this historic goal – the second of its kind since the eradication of small pox almost three decades ago – the world spotlight shines hot on Afghanistan and Pakistan as these countries work to take the world across the finish line.
In both countries, the redoubling of anti-polio efforts has seen some impressive gains. However, challenges remain. In spite of regular mass vaccination campaigns in both countries, reaching persistently missed children with oral polio vaccine (OPV) and delivering quality health services remain big challenges. In Afghanistan, conflict, difficult terrain and insecurity continue to hamper access, creating and sustaining reservoirs of poliovirus transmission, yet the programme maintains its neutrality to ensure the support of all key actors and to achieve the best results for children. In Pakistan, high population movement into areas where the virus remains and pockets of under-immunized children also continue to pose risks for viral transmission.
To improve the quality of campaigns and the public acceptance of the importance of vaccination, WHO and the partners of the GPEI – UNICEF, Rotary International, the Centres for Disease Control and Prevention and the Bill and Melinda Gates Foundation – are working closely with both national governments and community leaders to boost demand for OPV, and dispel false rumours surrounding the vaccine.
“The polio programme is not only engaging health officials and professionals, but also rallying the support of senior, influential religious scholars to reach out to communities,” said Dr Richard Peeperkorn, WHO Representative in Afghanistan. “A recent Ulama conference in Kabul brought together religious leaders from around Afghanistan, resulting in a public declaration encouraging caregivers to vaccinate children against polio and other vaccine-preventable diseases. Ulama conferences will be organised in five regions in the coming months to further strengthen the advocacy role of religious leaders in the fight against polio,” he explained.
WHO, along with partners, currently supports the training of 65,000 Afghan frontline polio workers on a newly-revised curriculum to enhance their skills in vaccination, surveillance for cases of acute flaccid paralysis, campaign monitoring and inter-personal communications. Frontline workers are trusted community members who care about the children in their communities, maximizing their ability to play a crucial role in the final push to eradicate polio.
In Pakistan, publicity campaigns to foster community trust and protection for polio vaccinators is helping to improve coverage in areas with clusters of refusals. “Although refusals are not a widespread issue in Pakistan, overcoming them where they are a problem is necessary for eradication,” said Dr Michel J. J. Thieren, WHO Representative in Pakistan. “WHO is supporting the Government of Pakistan and other partners to show that vaccinators are at the heart of every community and eradication efforts. Vaccinators are trusted and accepted by their community, which is helping the polio programme to encourage the vaccine seeking behaviour of parents,” he said.
In addition to advocacy and community outreach, WHO and partners in both countries are working constantly to fine-tune logistics to reach more children in campaigns. Revisions to Afghanistan’s ‘revisit strategy’ and the installation of fixed vaccination teams at Afghanistan-Pakistan border crossing points has helped to reach children on the move.
“Vaccination teams are re-visiting households with absent children at the end of every campaign day. There is also a revisit day at the end of each vaccination campaign on Fridays to reach out to families at picnics, public markets and mosques, to give OPV drops to children who may not have been at home when the teams first visited,” said Peeperkorn. “This type of ‘mop-up’ activity has been very effective in reducing the number of missed children,” he said.
“The proximity of the two countries makes polio importation a constant challenge,” said Thieren. “There is a large population of children under five that travel across the border which has led to shared WPV circulation in the two corridors with a Ping-Pong phenomenon between the bordering areas of the two countries. One of the strategies to reduce cross-border transmission by high risk mobile populations is to ensure vaccination teams are positioned in areas where there is huge population movement,” he added.
Afghanistan is also revising its microplans to obtain critical data on the size and location of target populations in different areas. Revised and accurate microplans are the backbone of successful polio vaccination campaigns as they determine the amount of vaccines that is needed, the number of health workers required and transportation needs, ensuring that every single child is reached by the polio vaccination teams.
Despite the gains, there is still much to be done, not only in Afghanistan and Pakistan but also in countries with declining immunization rates. So long as polio continues to circulate anywhere, children everywhere are at risk.
“We cannot afford to take our foot off the pedal now,” said Maher. “WHO and the GPEI partners will continue to support these two countries to get the job done. The broader support of the international community must also not waver,” he added.
Afghanistan and Pakistan will hold their next national vaccination campaigns in May. This year, there have only been 12 cases of polio, down from 23 cases in the same period for 2015.
Vaccinating children at a railway station in Quetta. UNICEF/PAK2015/Waseem Niaz
January 29, Islamabad: Pakistan’s polio eradication initiative has been put under the microscope by members of the Technical Advisory Group (TAG) in Islamabad this week as they review recent progress made in the fight to eradicate the disease from one of the world’s last reservoirs.
TAG Chair Jean Marc Olive said Pakistan colleagues presented TAG with a comprehensive picture of the epidemiological situation across the country, indicating that the initiatives and interventions that are being used show the country is on the right track to end transmission.
“In spite of this, we still have areas that could risk it all. Not only the Kyber-Peshawar-Nahangar corridor as highlighted by the Independent Monitoring Board , but in Karachi we have another hub of transmission. We need to put the maximum energy into Karachi.”
“If we increase our sensitivity, move closer to the ground with our interventions and focus more and more on the small scale, Pakistan will make it. I am confident of that.”