Port Sudan, Sudan – Sudan’s Federal Ministry of Health (FMOH) will launch a polio vaccination campaign in April 2024 in response to a new emergence of variant poliovirus type 2 reported in January 2024. It was detected in six wastewater samples collected from September 2023 to January 2024 in the Port Sudan locality, Red Sea State.
The FMOH, with support from the World Health Organization (WHO), has completed field investigations and a risk assessment to determine the extent of the virus circulation. Preparations for a polio vaccination campaign in April 2024 in Red Sea, Kassala, Gedaref, River Nile, Northern, White Nile, Blue Nile and Sennar states are under way, with a differentiated approach for the rest of the states as conditions allow.
One of the first tasks they took on was to find ways to detect the possible spread of an outbreak of variant poliovirus that was confirmed in December 2022 after a paralysed child living near the border with Chad tested positive for the virus. Immediately after the start of the conflict, they worked to maintain the essential function of surveillance for acute flaccid paralysis (AFP) – the most common symptom of polio – in children.
Prioritizing essential polio functions
Much like a relay race, in AFP surveillance, speed and coordination are key. Once health teams find a child with AFP, the race begins. But emergencies often present additional hurdles. In one of the localities in Sudan’s White Nile state, Ahmed Masaood, a health worker, was tasked with collecting two stool samples from a child presenting with AFP. However, when the roads outside turned unsafe during Ahmed’s visit, he ended up having to seek refuge with the family he was visiting for two nights. As soon as he could, he rushed to the state cold room with his stool carrier to drop off the samples for storage until they could be tested.
The next lap of the race involves getting children’s stool samples to a WHO-accredited laboratory for testing. Due to the conflict, Sudan’s polio laboratory is not functioning, which meant the polio programme urgently needed to look for another laboratory to test stool samples to determine if children presenting with AFP had indeed been infected with poliovirus.
In a remarkable partnership, Sudan’s polio programme teamed up with Egypt’s health authorities to use the VACSERA laboratory in Giza for this crucial task. Senior decision makers at the Egyptian Ministry of Health not only approved the collaboration but instructed for it to begin as soon as possible.
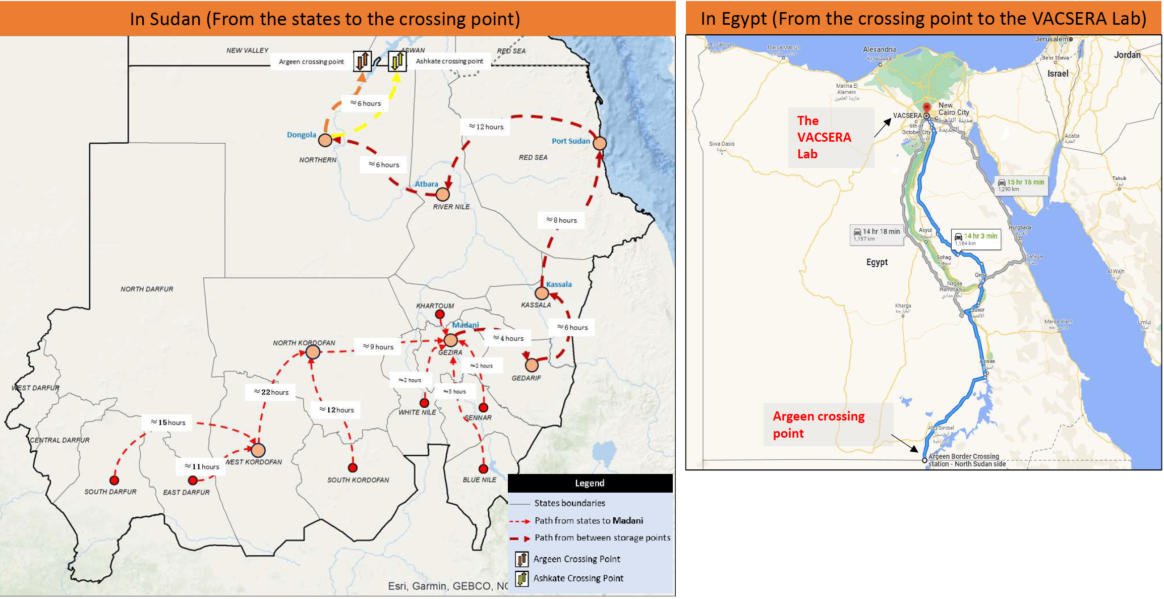
In June, the polio programme in Sudan completed a pilot mission to transport stool samples to the VACSERA laboratory for testing. With the conflict impacting movement and security on the roads, creativity was required to get the samples from collection points identified, such as Gezira to Port Sudan to Dongola, all the way to the border. Throughout, health workers relied on two criteria to ensure safe passage for themselves and their cargo: first, their neutrality, and second, their status in communities. The health workers who made this happen are known to and trusted by the communities they serve, and that trust, in many cases built over decades, facilitated their travel by road.
The first shipment of stool carriers passed through five stops in different states following a pathway assessed for security considerations. In Red Sea state, Dr Thabit Mohammed Elsadig, a WHO Public Health Officer, spent three days pulling together all the resources drivers would need, from permits and security clearances to cash, fuel and food. As the situation was formally graded as a level three emergency, this triggered WHO’s Emergency Response Procedures, effectively enabling staff to respond and repurpose resources at speed. In some cases, Dr Thabit and others used their own resources to make things happen.
At each stop, health workers picked up more stool samplesfrom their colleagues. They checkedtemperature controls in the sample carrier and replaced old ice packs with fresh ones to maintaintemperature and handling protocols of the reverse cold chain.
With the occupation of the National Public Health Lab in Khartoum by one of the parties, Hatim Babiker Othman, National Coordinator for the Polio Lab in Sudan, moved to Port Sudan during the first month of the conflict and started to restructure the polio lab’s functions. He organized samples in small boxes, assigned lab numbers, and established effective communication with the focal point in Egypt, to coordinate the handover of samples. Hatim traveled with the samples from Port Sudan to Atbara, Dongola, and finally, the Argeen border crossing point.
Meanwhile, WHO colleagues contacted the Egyptian Ministry of Health to confirm that, at last, the samples were on their way to the border. At the Argeen Gate, border officials examined the boxes and their contents. Dr Thabit recalled thinking that if anything went wrong at this point, all their efforts – days of planning and transport by road – would have gone to waste.
“The sample carriers were like trunks of gold for us. We hoped they would treat them well, and they did,” he said, with reference to their value in signaling any epidemiological developments related to the ongoing variant poliovirus outbreak.
Exemplary inter-country support
Once they received a prompt from WHO, a team from Egypt’s Aswan Governorate of Health set out on a six-hour journey to the shared border. There, they collected the samples and headed back to the health facility in Aswan for more fresh ice packs before driving to the VACSERA laboratory in Giza, a 14-hour drive away. The entire journey from Madani, Sudan, to Giza, Egypt, can take up to 56 hours and demands absolute precision in planning and execution.
Acknowledging Egypt’s generous support, Dr Ni’ma Saeed Abid, WHO’s Representative in Sudan said, “Our partners in Egypt have demonstrated how stronginter-country collaboration can help in ending diseases. We remain grateful to them for their timely support, and to every link in this chain of coordination. This support is a demonstration of ‘delivering as one WHO’.”
On 16 June 2023, VACSERA received a shipment of 56 stool samples for testing for poliovirus.Lab personnel prioritized Sudan’s samples for immediate testing, and the testing process began on the day of arrival.Final results were shared in 11 days — a full 10 days less than the standard three weeks. The results were also good news: no sample tested positive for variant poliovirus.
“Our heroic health workers stayed to deliver our mandate and support the most vulnerable communities in the face of the ongoing conflict,” Dr Nima said. “They are continuously finding extraordinary solutions to continue to protect children from polio and other vaccine-preventable diseases. This is a lesson to be followed by the integrated disease surveillance team. It reinforces what we believe in:everything is possible, with strong determination and will.”
Two technical assessment missions worked on scrutinizing available evidence and analyzing the absence of polioviruses across Sudan. The first mission, conducted virtually in October 2021, shared their recommendations with Sudan’s polio eradication team to ramp up their efforts across the country.
A second official outbreak response assessment team undertook the next phase of this detailed task. They visited Khartoum and six of Sudan’s 18 states as part of their work from 24 July to 1 August 2022.
Both review teams comprised experts from the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF). Their skills and experience ranged from global public health, epidemiology and biostatistics to surveillance, vaccine management and communication.
They worked hand in hand with the Federal Ministry of Health of Sudan, with state-level ministry staff and with health workers at ground level.
After a close review of the functionality and sensitivity of the country’s surveillance system, the assessment team noted that Sudan’s acute flaccid paralysis (AFP) surveillance indicators are indeed meeting the necessary standards. The gold standard for polio surveillance is through searching for AFP in children, and testing stool samples to confirm the presence of the virus.
All poliovirus samples collected since 18 December 2020, the date of onset of paralysis of the last child affected in the outbreak, were processed like clockwork in Sudan’s laboratory. They were reported as poliovirus negative and recorded.
The missions noted Sudan’s 14 environmental surveillance sites are also collecting and testing waste water samples regularly, in line with international protocol.
During the polio outbreak, 14 sewage samples in the country’s bustling capital, Khartoum, tested positive for cVDPV2, indicating circulation there.
As part of their work, the technical mission also reviewed the core functions of Sudan’s laboratories and the country’s preparation mechanisms for poliovirus events or outbreaks. This also included data on population immunity, childhood immunization and vaccine management protocol.
A large part of Sudan’s success can be attributed to its swift response to the outbreak as soon as it was confirmed.
The country conducted two high-quality nationwide campaigns in all 18 states to curb virus spread in November 2020 and January 2021. Each campaign delivered monovalent oral polio vaccine type 2 (mOPV2) to over 8 million under-fives.
Weighing in on this milestone, senior experts in WHO’s polio eradication programme, including
Dr Hamid Jafari, WHO Director for Polio Eradication in the Eastern Mediterranean Region, and Dr Ni’ma Saeed Abid, WHO Representative to Sudan, lauded public health officials and immunization health workers on the ground for their swift response to the outbreak.
They reiterated the importance of maintaining sensitive AFP surveillance, ensuring better outbreak preparedness and response, enhancing coverage of essential immunization, and strengthening cross-border coordination. This is crucial given Sudan remains at high risk of importation of polioviruses.
Following this extensive work, the outbreak response assessment team concluded that the spread of cVDPV2 has indeed stopped, and that the outbreak is over.
Dr Niazy trains medical staff on handwashing during a COVID-19 training session in River Nile state. Credit: WHO-POL/Sudan
The polio eradication programme has stepped up to help the Sudanese Ministry of Health limit spread of the COVID-19 virus. The programme is working in 14 states in the country supporting COVID-19 surveillance, information dissemination and training of health workers.
Dr Niazy Abd Alhameed Abd Alwahab, a National Medical Officer for the polio programme since 2013, is one of the personnel playing a key role. He and colleagues recently led two WHO COVID-19 trainings in River Nile state, one for Rapid Response Teams (RRTs) and one for local hospital staff, in addition to supporting trainings run by the State Ministry of Health.
Thanks to the trainings, health workers in all seven localities in the state are ready to help individuals who are showing symptoms of COVID-19. In total, more than 3000 RRT members have been trained across Sudan with support from polio National Medical Officers.
By early May, River Nile state had suffered seven cases of COVID-19, with two fatalities. “The state is organized to respond”, Dr Niazy explains, “All patients are being treated in dedicated isolation facilities in hospitals, and medical staff are on high alert for more cases. We helped train teams so that they are able to serve the population.”
Training Rapid Response Teams
A five-day training of Rapid Response Teams, funded by WHO, was targeted at seven teams, one from each state locality. Of the 42 individuals trained, 30 were women and 12 were men. The Rapid Response Teams have been created for the COVID-19 response. Each team contains individuals with the collective public health experience to contribute to local efforts to fight the virus, spearheading work in contact tracing and engagement with the community.
The first day of training was attended by the Director General Health of the State Ministry of Health and the Head of the Emergency Humanitarian Assistance (EHA) department.
Dr Niazy explains that over the five days, participants gained a comprehensive understanding of Sudan’s COVID-19 surveillance and contact tracing systems, infection prevention and control practices, case management methods, and how to collect samples and arrange shipment to the national laboratory in Khartoum. Participants were also trained on how to use PPE safely and how best to wash their hands.
“Participants were encouraged to take part in interactive exercises to test and strengthen their knowledge, as well as take part in discussions,” he says.
“By the end of the training, all participants were fully trained and able to pass on their knowledge in their localities.”
Training local health staff
The polio programme also supported a two-day COVID-19 training for 34 women and 22 men who work in state hospitals as doctors, lab technicians, or other medical personnel. The programme continues to support the State Ministry of Health with further local trainings, including for medical registrars.
Ongoing challenges
The situation in River Nile state is very challenging. There are chronic shortages of PPE, hand sanitizer and masks, and WHO is offering urgent support to help procure these. Severe shortages of fuel and currency are making response more difficult. Social norms in some communities dissuade individuals with COVID-19 symptoms from seeking medical assistance, and work must be carried out to build trust and ensure people with COVID-19 are found and offered care.
To serve the COVID-19 response and prevent virus spread, the polio eradication programme has had to scale back some of its usual work. Dr Niazy explains, “Vaccination campaigns are paused, and many private clinics are closed, some of the public health centres are turned into isolation centres as part of the response to this emergency. This makes detecting acute flaccid paralysis (AFP) more difficult, as health personnel are trained to report children with AFP who come to the health centres.”
Efforts are being made across the Eastern Mediterranean Region to minimize the impact of COVID-19 on the overall health of populations, during a time when many health activities cannot go ahead. In Sudan, a number of children do not have full immunity against polio, and it is critical that routine immunization continues where possible until vaccination campaigns resume.
Dr Hoda Youssef Atta, WHO Representative a,i, explains, “During the COVID-19 emergency the polio eradication programme is committed to providing expertise, training and medical skills to protect Sudan. However, as soon as it is safe to do so, we must scale up programme operations once more to protect vulnerable populations from polio.”
Sudan borders a number of countries facing outbreaks of circulating vaccine-derived poliovirus, including Chad and the Central African Republic (CAR) to the west, and Ethiopia and Somalia to the east. Population movements between these countries increase the risk of importation of polio to Sudan. The World Health Organization and national health authorities in Sudan are scaling up efforts to reduce the risk of poliovirus transmission to the country.
To prevent a possible outbreak, health authorities have been working amidst immense operational challenges to carry out vaccination campaigns and strengthen disease surveillance. Public health teams in Sudan and CAR are collaborating to share details of vaccinated refugee children with their country of origin, and exchange information on upcoming supplementary immunization activities and reported cases of Acute Flaccid Paralysis.
Sudan was declared free of wild poliovirus in 2015, but remains at considerable risk for poliovirus importation or a VDPV outbreak. Much of the risk is shaped by Sudan’s unique population dynamics, and by the devastating effect of population movement, conflict and instability affecting routine immunization. Additionally, nomads, who account for around 10% of Sudan’s population, regularly move across borders to graze animals in Chad and CAR.
Over 8 million children under the age of five are estimated to live in Sudan – an age group considered to be most vulnerable to contracting and being paralyzed by poliovirus. Sudan also has large numbers of internally displaced people and refugees, many in the areas of the country with the lowest levels of routine immunization, such as the Darfur region.
In September and October 2019, states on the border between Sudan and CAR implemented accelerated routine immunization to provide children with coverage against a variety of vaccine-preventable diseases. Teams conducted reviews of vaccination facilities and posts in border areas, and orientation sessions were held in healthcare settings to reinforce reporting cases of Acute Flaccid Paralysis. Children received oral polio vaccine, pentavalent vaccine, and inactivated polio vaccine. Initial data from the campaigns suggests a spike in coverage, with teams reaching many children previously unprotected.
As the world inches closer towards a polio-free future, finding and closing remaining gaps in national health system capacities to pick up traces of the poliovirus is critical. Only three countries remain on the global endemic list – Afghanistan, Pakistan and Nigeria – but the threat of poliovirus resurgence remains very real, particularly for countries with a history of importation of poliovirus from these endemic areas.
In order to ensure that surveillance systems in these ‘at-risk’ countries are up-to-scratch and sensitive enough to adequately detect and report cases of acute flaccid paralysis (AFP) – a major indicator for polio – the World Health Organization regularly leads expert reviews to put systems under the microscope.
Expert review in Sudan
Eighteen technical officers and polio surveillance experts from WHO, UNICEF, the U.S. Centers for Disease Control and Prevention, the Bill & Melinda Gates Foundation and the Eastern Mediterranean Public Health Network recently met with Ministry of Health staff in Khartoum to share their findings and recommendations after scrutinizing Sudan’s surveillance performance at federal and state levels.
“Sudan has not seen a case of polio for almost nine years, however, certain factors put it at considerable risk of poliovirus importation and outbreaks,” said Dr Naeema Al Gasseer, WHO Representative to Sudan. “It is very important that the country remains on guard against polio and continually analyses and improves the quality of its AFP surveillance, particularly in the high risk areas,” she said.
“Strong AFP surveillance is a cornerstone of the polio eradication effort ̶ it enables us to quickly pick up poliovirus if it is circulating and react with an appropriate response,” said Dr Ni’ma Abid, a senior technical expert from WHO’s regional polio eradication hub in Amman, Jordan. “There is no margin for error and in at-risk countries facing such challenges as Sudan, we need to thoroughly examine AFP surveillance systems to make sure that they are sensitive and fast enough to detect transmission. This is a practice that will need to continue even after the world is certified polio-free,” he added.
Risk factors and special strategies
Sudan is the third largest country in Africa and home to over 40 million people. Insecurity, forced displacement, frequent nomadic population movement and inaccessibility in some areas make it challenging for health workers to consistently reach all children with vaccines to build immunity. Refugee influxes across porous borders with conflict-affected neighbouring countries exacerbate the risk of disease and compound pressures on the country’s already stretched health system. In addition, high sub-Saharan temperatures and rough expansive terrain can make timely collection and transportation of stool specimens from children with AFP for laboratory testing difficult.
Special strategies have been devised to cater for the specific surveillance challenges associated with reaching high risk groups. Examples include active searches for AFP cases and sample collection by community-based surveillance officers in areas with access issues, the mapping of the movement of displaced populations, and establishing regular communication with nomadic community focal points who report AFP cases via mobile phone. In refugee camps, vaccination posts have provided an opportunity to screen for children with AFP, and collaboration and sensitization of non-government organization (NGO) staff has helped to improve reporting of AFP cases.
Eighteen states were assessed throughout the review, with visits to 90 health facilities, the families of 16 children with AFP, and high-risk special populations. Overall conclusions were that the system is meeting global AFP surveillance targets and it is unlikely for polio to circulate undetected. However, gaps were identified that need to be addressed.
“Surveillance system performance in Sudan is sensitive and we were pleased to see implementation of the recommendations made at the last review,” said Dr Abid. “However, more attention needs to be paid to surveillance in refugee communities, cross-border population movement, and programmatic issues such as the high level of turnover of national surveillance staff,” he said. “We encourage the government of Sudan to implement the recommendations made at the review to address these and other gaps,” he said.
“WHO and partners commend the government of Sudan for its efforts to date, and stand ready to advise and support to keep the country polio-free,” said Dr Al Gasseer. “Until polio is gone for good, globally, we must make every endeavor to prevent resurgence,” she said.
Sudan witnessed its last case of indigenous wild poliovirus in 2001. Since then it has been exposed to several wild polio importations from Chad and Ethiopia with its most recent case in March 2009.
It starts with a sick child, whose arms or legs have suddenly become weak and floppy. A trip to the local health centre, which could be many miles away, confirms that the child is showing classic signs of acute flaccid paralysis. This is one of the key indicators for poliovirus and kick starts the polio surveillance system into action. In Sudan, an innovative approach to transporting stool samples from potential polio cases to the laboratory for testing is making it even more likely that if polio returns, it will be found.
Strong surveillance to identify every case of acute flaccid paralysis is the golden standard of the polio eradication programme. In countries like Sudan, where the last case of wild poliovirus was seen in March 2009, it remains critical. Even though Sudan is now polio-free, it remains at risk of reimporting the virus, so a high level of vigilance is needed while polio continues to circulate anywhere in the world.
The importance of strong surveillance in Sudan
Amid outbreaks of acute watery diarrhoea, severe malnutrition in children under 5, large scale internal population displacement and an influx of more than 1 million refugees from South Sudan due to conflict, Sudan has managed to maintain a strong surveillance system for polio. Despite these challenges, global surveillance standards – which tell a country whether their system is sensitive enough to catch polio circulating in communities – continue to be met.
But polio remains a threat to every child, everywhere, until it is stopped for good. Today, only three countries remain to be polio endemic – Pakistan, Afghanistan and Nigeria. Countries like Sudan that are close by, with low routine immunization rates, weak health infrastructure or facing conflict and population displacement, remain at a higher risk of polio finding its way back.
The role of the reverse cold chain for surveillance
When any case of acute flaccid paralysis is found anywhere in the world, stool samples from the affected child must be transported carefully to the laboratory so that they can be tested to identify whether the poliovirus was the cause.
Mr Jaouad Tilout, from WHO Eastern Mediterranean Office Polio Eradication Programme, explains that this journey undertaken by each sample is known as the ‘reverse cold chain’. “If a cold chain is what you call the transport chain that goes from a laboratory to the field – where vaccines must be kept at a certain temperature from the moment they are produced, until they are administered in order for them to work – a reverse cold chain is the process of stool samples that need to be tested getting back to the lab from the field at a certain temperatures so that the virus that might be in the sample will still be identifiable.”
Innovations in the reverse cold chain
With support from Global Polio Eradication partners, Sudan is part of a pilot study of a new device that aims to ensure stool samples collected from acute flaccid paralysis cases reach Sudan’s National Poliovirus Laboratory in the right condition for effective testing.
Mr Jaouad Tilout says that the pilot study aims to assess whether specimens being transported are meeting global guidelines and introduce continual temperature recording probes known as ‘LogTags’ to track specimens during their journey to the lab.
Dr Christopher Hsu, from the Centers for Disease Control (CDC), and Mr Tilout co-led a two-day workshop in Khartoum to train public health staff on the use of the new tool.
“This is a really important innovation that could be implemented in other EMRO countries, such as Yemen and Somalia, to assess their reverse cold-chain too. It’s a critical process in the end game for polio because we are looking to keep any potential poliovirus alive in the stool specimen so it can be properly notified by the lab,” Mr Tilout says.
The LogTag training has been delivered to 20 health staff from Sudan’s National and State health offices, the National Polio Laboratory, and the WHO Sudan Country Office. The study will be conducted over the next six to 12 months with the goal of collecting approximately 250-300 LogTag measurements. Findings from this assessment will be used to give feedback to state polio surveillance officers on any deviation from reverse cold-chain parameters.
Oral polio vaccine is stored in refrigerators at a health facility. The rainy season has flooded the area but the refrigerators are intact, keeping the vaccine chilled.
A child is given the vaccine at the Torti camp for internally displaced people. Frequent travel between Chad and Sudan makes it easy for the poliovirus to spread. In the Darfur region, displaced children are particularly vulnerable.
Dr Salah Haithami of WHO checks that a vaccinator knows her tasks – giving two drops of vaccine to every child, marking their fingers with indelible ink, and storing the vaccine safely in her cooler box.
Dr Tayeb EL Saied, in charge of Sudan's immunization programme, demonstrates house marking. These marks tell vaccination teams and monitors whether a house has been visited and whether the children under five years of age have been vaccinated.
A team of vaccinators waits to be driven out to a remote community. More than 90% of vaccinators are women, as only women have access to private households.