
July 2009, no.4
Polio Research Committee outcomes, call for research proposals, India vaccine trials prompt major strategic shift, unmet research needs.
Articles
The third meeting of the Polio Research Committee (PRC) convened in Geneva, Switzerland on 2–3 June 2009. Discussions focused on various ongoing and proposed research topics relating to both the pre- and post-eradication era. Reviewed research topics included:
- addressing compromised oral polio vaccine (OPV) efficacy (e.g. zinc supplementation to improve OPV efficacy; zinc has been shown to be associated with a reduction of diarrhoeal disease)
- developing ‘affordable’ inactivated polio vaccine (IPV) options (e.g. IPV production from non-infectious seed strains, adjuvants and Sabin-IPV development)
- use of IPV in northern India to fill residual immunity gaps among very young children and enhancing surveillance for acute flaccid paralysis (AFP).
In its deliberations, the PRC endorsed the following external research proposals for funding:
Antiviral drug development:
The proposal is to identify new antiviral compounds against polioviruses through industrial-scale mass screening of compounds and evaluation of candidate compounds in vitro and in mouse models.
Assessment of alternate polio strains for vaccine production:
This project will create efficient poliovirus packaging cell lines and produce encapsidated poliovirus replicons as seed material for IPV production. Those replicons lack the capsid encoding genome segment, and are therefore unable to form virus particles. Additionally, replicons are considered to be identical in antigenicity, stability and biophysical properties to wild polio virus.
Impact of zinc supplementation on OPV efficacy:
This proposal will investigate whether low zinc status in infants contributes to diminished immune response to OPV; and, evaluate the impact of zinc supplementation among infants on immune response to OPV.
The next PRC meeting is scheduled for 10–11 November in Geneva, and will focus on pre-eradication issues, low vaccine efficacy and risk factors contributing to low vaccination coverage.
A recently-completed multi-centre clinical trial in India (Chennai, Indore, and Pune), sponsored by Panacea Biotec Ltd, initiated based on a recommendation by the Advisory Committee on Poliomyelitis Eradication (ACPE) and with extensive technical and financial support by the World Health Organization (WHO), has demonstrated the non-inferiority of a bivalent (types 1 + 3) oral poliovirus vaccine (bOPV) compared with monovalent type 1 oral poliovirus vaccine (mOPV1) and monovalent type 3 oral poliovirus vaccine (mOPV3).
The trial also demonstrated the superiority of bOPV compared to the respective Sabin type 1 and 3 strains contained in the trivalent oral poliovirus vaccine (tOPV). Immediately after the trial results were available, the ACPE convened by conference call and reviewed the trial outcomes and current epidemiology of wild poliovirus globally. It concluded that the use of bOPV in supplementary immunization activities (SIAs) constitutes and important new tool for the Global Polio Eradication Initiative to complement the use of tOPV for routine immunization and SIAs as well as the use of mOPVs in SIAs. The clinical trial report was made available in July 2009 by the sponsor to other manufacturers interested in bOPV production.
To date, at least four manufacturers are seeking national licensure for bOPV and a process has been initiated to review in parallel the regulatory dossiers for WHO-prequalification of these products for United Nations purchase. It is anticipated that the first newly-licensed bOPV could be used in supplemental immunization activities as early as November 2009.
In addition, the Global Polio Eradication Initiative is also awaiting the results of another clinical trial that was conducted in Moradabad district, western Uttar Pradesh, India. The trial evaluated five arms, a regular- and higher-potency mOPV1 and three inactivated poliovirus vaccine (IPV) arms. Unprecedented collaboration by Panacea Biotec Ltd, the sponsor (with IPV-bulk supplied by the Netherlands Vaccine Institute), GlaxoSmithKline, and Sanofi Pasteur made the trial possible. The results of this trial should be available in mid-September 2009 and should answer the following questions:
- Is higher-potency mOPV1 more immunogenic than regular-potency mOPV1 in northern India?
- Does IPV have a role to play in closing remaining immunity gaps?
- Will a fractional dose of IPV (1/5th of a full dose) given intramuscularly by needle-free device perform as well as a full dose of IPV?
As with the case of bOPV, the ACPE will review the data on higher-potency mOPV1 and on full- and fractional-dose IPV as soon as these will be available. It is expected, depending on the outcome of this trial, that major strategic shifts in the use of these products should be anticipated (as is the case with bOPV). These clinical trials will help inform the finalization of the new Global Polio Eradication Initiative five-year Strategic Plan (expected for publication in January 2010).
Global post-eradication IPV supply and demand assessment conducted
The Bill & Melinda Gates Foundation, in discussion with the World Health Organization, commissioned an assessment of global post-eradication inactivated polio vaccine (IPV) supply and demand, with a focus on identifying supply strategy implications for developing world populations. The insights and conclusions from this assessment were intended to help inform policy and aid country decision making.
The assessment was completed by Oliver Wyman, an international management consulting firm, over a ten month period and involved numerous consultations with existing and potential IPV suppliers as well as demand experts. A paper summarizing the assessment’s findings was released in March.
In the paper, the authors define future demand scenarios for IPV use, characterize the current and evolving supply base, and recommend a path forward to ensure access for developing world populations.
Related links
Global post-eradication IPV supply and demand assessment: integrated findings [pdf 179kb]
Commissioned by the Bill and Melinda Gates Foundation, prepared by Oliver Wyman Inc
March 2009
Conflict in Afghanistan and Pakistan has made efforts to immunize children more difficult and perilous for health workers and citizens alike. Although polio workers are not often directly targeted, in areas of active conflict polio eradication partners face immense challenges in extending services without compromising the safety of the immunization workers.
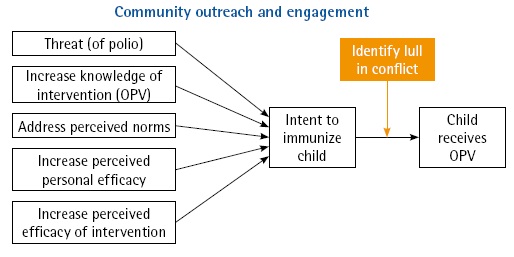
In this type of environment, polio teams have looked to define ways to take advantage of quiet periods when fighting has abated, and to encourage people to be more pro-active in immunizing their children whenever an opportunity exists. One strategy relies on opportunistic immunization that occurs when polio workers see a lull in fighting in an area that was previously inaccessible, and then quickly marshal their forces to immunize children in those communities.
To succeed, it is critical to ensure child caregivers receive information on the need to immunize their children and of immunization services. To help increase this awareness requires local leadership to own and actively support polio eradication efforts. Local leaders can inform polio workers of lulls in conflict, and also use local networks to inform people in communities about available immunization services.
The demand for oral polio vaccine (OPV) is further driven by the deployment of local social mobilizers who work with communities to help them understand the threat of polio and the necessity of immunization, both during supplementary immunization activities (SIAs) and routine immunization.
 |
A key innovative strategy in place to further drive this demand is the ‘courtyard women strategy’. This activity brings trained female health workers into compounds to meet with mothers and other female child caregivers to engage in guided discussions about polio eradication, routine immunization and other basic child survival topics. As mothers are the primary caregivers of young children (the most vulnerable to polio), it is essential to increase an understanding among this target group of the need to immunize and increase empowerment to ensure children receive OPV and other vaccines. In areas where the ‘courtyard women strategy’ has been put in place, there is evidence that routine immunization and coverage during polio SIAs has increased.
Reigns APK