JICA continues to support Pakistan in polio eradication efforts
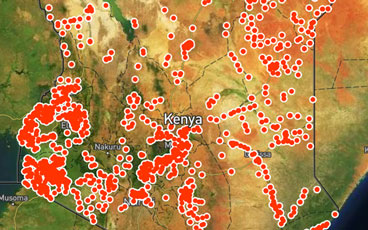
With no wild poliovirus reported anywhere in Africa since 2016, efforts are being intensified to actively look for the virus, to ensure it i...
February 2019, Brazzaville, Republic of Congo
WHO Executive Board’s strong push to finish the job
Progress in the challenging last mile of eradication
Following confirmation of circulating vaccine-derived poliovirus type 2 (cVDPV2) on 8 January 2019, planning for an outbreak response is und...
As the Global Polio Eradication Initiative (GPEI) enters its 31st year, the Chairs of the effort’s main global advisory bodies issue an extr...
In the Horn of Africa polio outbreak, immunization efforts are focusing on a group known as “special populations”.
Jean-Marc Olivé, Chairman of the Technical Advisory Group, reflects on what needs to be done to end polio in the Horn of Africa.
To truly ensure no child is left behind, the Global Polio Eradication Initiative is reaching out to some of the most remote communities in t...
A review committee met in Nairobi to assess progress of the African region towards being certified polio-free
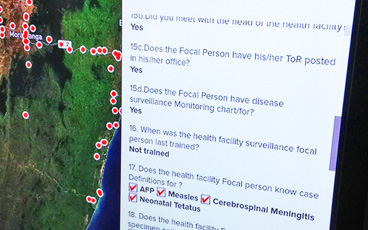
In the Horn of Africa, health workers are using application-based technology to respond to poliovirus outbreaks with greater speed and accur...
Meet WHO’s Chris Maher, who has spent 25 years following polio to its last hiding places.
The innovations making a difference to outbreak response.
Take a look at how the Papua New Guinea Government, the World Health Organization, and partners of the Global Polio Eradication Initiative a...
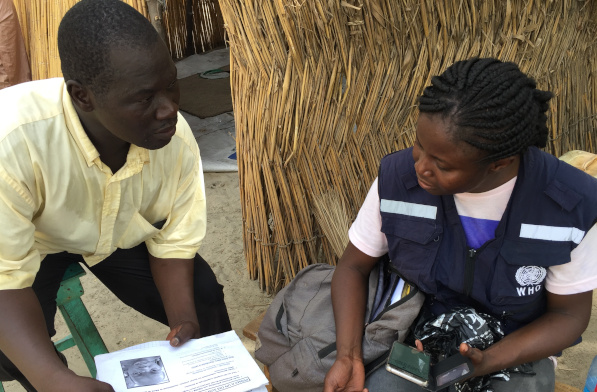
Across the Lake Chad Basin, e-Surve technology is revolutionizing the way that the polio programme conducts disease surveillance
In Iraq, polio vaccinators work to protect conflict-affected children.
Towards a polio-free Africa: A chat with Professor Rose Leke, Chair of the African Regional Certification Commission.
La Dre Adele Daleke Lisi Aluma s’efforce d’atteindre les enfants jamais vaccinés
In Pakistan and across the world, the poliovirus surveillance system and laboratory network are critical to eradication efforts.
In Nigeria, experts from the frontline of polio eradication are helping to end other disease outbreaks.
Dr Adele Daleke Lisi Aluma works to reach children who have never been vaccinated
US$ 3.2 million pledged for equipment to help detect the last remaining reservoirs of the virus.
The strong polio eradication infrastructure in Borno is supporting Nigeria to vaccinate over eight million people against yellow fever.
The polio surveillance system is finding the virus in the most challenging areas so that children can be protected and polio stopped for goo...