After the safe and successful rollout of nationwide polio campaigns since November 2021, we have received tragic news that 8 health workers at the forefront have been killed this morning in a series of shootings in Takhar and Kunduz in northeast Afghanistan. The vaccination campaign has been suspended in both provinces.
A statement has been issued by the Regional Director of WHO’s Eastern Mediterranean Region, Dr Ahmed Al-Mandhari, as well as by the United Nations in the country, condemning these attacks, expressing condolences to the families and underscoring that the provision of health and the safety of healthworkers at the forefront are paramount, and must be kept neutral to any geo-political situation anywhere.
Our thoughts and prayers are both with the families and our teams on the ground at this time.
Cairo, 10 February 2022 – The fourth meeting of the Regional Subcommittee on Polio Eradication and Outbreaks was convened on Wednesday 9 February, by WHO’s Regional Director for the Eastern Mediterranean Dr Ahmed Al-Mandhari. The meeting was attended by health ministers or their representatives from Djibouti, Egypt, the Islamic Republic of Iran, Pakistan, Qatar, Saudi Arabia, Sudan, United Arab Emirates and Yemen.
The Subcommittee declared the ongoing circulation of any strain of poliovirus in the Region to be a regional public health emergency and called on all authorities to enable uninterrupted access to the youngest and most vulnerable children through the resumption of house-to-house vaccination campaigns. It issued statements on wild poliovirus circulation in Afghanistan and Pakistan and on the circulation of vaccine-derived poliovirus strains in Yemen, where limits on house-to-house vaccination are preventing access to the most vulnerable children.
The spread of polio in the Eastern Mediterranean Region is a pressing emergency and it remains a Public Health Emergency of International Concern (PHEIC) under the International Health Regulations (IHR 2005).
Members noted a sharp decrease in cases of wild poliovirus in Afghanistan and Pakistan in 2021 but warned against complacency.
“Wild poliovirus transmission is at a historic low in the endemic countries of Afghanistan and Pakistan. The progress is remarkable, but it is fragile. The opportunity to end polio is knocking at our door, and we must seize it,” said Dr Al-Mandhari.
Speaking to the progress made in the last year, the Special Assistant to the Prime Minister on Health, Dr Faisal Sultan, assured members that the programme in Pakistan was leaving no stone unturned in the pursuit of zero polio transmission.
“We have intensified efforts in the hardest districts and core reservoirs and we are closely monitoring transmission across the border in coordination with Afghanistan, taking measures to respond to outbreaks if they occur and making every effort to ensure that the virus doesn’t spill over in either direction. To boost the confidence of marginalized communities, we are also providing essential services and vaccination of other antigens and diseases,” he said.
Outbreaks of circulating vaccine-derived polioviruses type 1 (cVDPV1) and type 2 (cVDPV2) continued to emerge and spread in the Region in 2021. As of February 2022, Afghanistan, Djibouti, Egypt, Pakistan, Somalia, Sudan and Yemen are responding to transmission of vaccine-derived polioviruses.
“The increasing outbreaks of circulating vaccine-derived poliovirus type 2 in the Eastern Mediterranean Region and neighbouring countries of Africa are deeply concerning and must be stopped rapidly. To do so, we need to ensure that we are creating an enabling environment for health workers to reach children with those two drops of polio vaccine,” said newly nominated co-chair H.E. Dr Hanan Mohamed Al Kuwari, Minister of Public Health of Qatar.
During the meeting, Djibouti’s Public Health Minister, Dr Ahmed Robleh Abdilleh, shared plans for vaccination campaigns and increased surveillance in response to the transmission of cVDPV2, recently detected through the newly launched environmental sampling programme.
Reflecting on the work of the Subcommittee, co-chair and Minister of Health and Prevention of the United Arab Emirates H.E. Abdul Rahman Mohammed Al Owais urged members to sustain the commitment seen in in 2021.
“We have together advocated for an increase in domestic funds, we have driven collaborative public health action in our own countries, and collectively pushed for a regional response to address the regional public health emergency of the poliovirus. But these things alone will not end transmission,” he said.
Dr Al-Mandhari expressed appreciation for Egypt’s role as the first country in the Region to roll out a nationwide vaccination campaign using the novel poliovirus vaccine, and Chris Elias, Chair of the Polio Oversight Board, praised the remarkable progress made in polio eradication in Pakistan with support of the United Arab Emirate’s Pakistan Assistance Programme.
“This regional solidarity and commitment we have seen, through this Subcommittee, is something I am proud of. It is this commitment to the end goal that will help push us over the last mile,” said Dr Hamid Jafari, director of the regional polio programme and co-facilitator of the Regional Subcommittee.
With the ongoing COVID-19 pandemic, continued wild polio transmission in the remaining endemic countries and spreading outbreaks of circulating vaccine-derived polioviruses type 2 (cVDPV2), this year began with many challenges facing polio eradication efforts. But amid this new reality, countries and partners of the Global Polio Eradication Initiative (GPEI) intensified their efforts to protect children from lifelong paralysis.
In June, the GPEI launched the new GPEI Strategy 2022-2026, which lays out the roadmap to achieving a lasting world free of all forms of polioviruses through stronger community engagement, a renewed focus on gender equity and the rollout of new tools and technologies. These new tools include the novel oral polio vaccine type 2 (nOPV2), which began deployment under Emergency Use Listing (EUL) as part of the GPEI’s broader polio vaccine repository to curb cVDPV2 transmission. In August, the WHO African Region celebrated one year since it was certified wild polio-free, and countries recommitted to strong cVDPV2 outbreak response across the continent with the support of the GPEI.
Further critical progress took place in Afghanistan – one of two final countries endemic for wild poliovirus, along with Pakistan. For the first time in more than three years, nationwide polio immunization campaigns resumed across Afghanistan reaching 8.5 million children, including 2.4 million children who were previously inaccessible.
At the same time, polio programme health workers at the forefront continued to support global COVID-19 response efforts by delivering vaccines, mobilizing communities, and countering misinformation among other activities. The use of GPEI infrastructure for health emergency response has provided critical lessons for integrating polio resources into broader health systems as more countries work towards transition and the post-certification period.
Following dire predictions issued at the end of 2020, the polio programme once again proved its ability to adapt to programmatic, epidemiological and political developments. Entering 2022, there is much cause for cautious optimism – wild poliovirus transmission has slowed drastically, and cases of cVDPV2 have also declined compared to last year.
Importantly, commitment to achieving a lasting polio-free world is evident at all levels: by core GPEI partners, including among the Polio Oversight Board, which travelled to Pakistan twice in 2021; by health workers, communities and parents; and by country leaders worldwide who helped champion this year’s milestones. With the new strategy, new tools and adapted approaches, the stage is set to achieve lasting success.
To stop all forms of polio for good, the GPEI aims to capitalize on the positive epidemiological situation leading into 2022. A key opportunity to kick-start the year will be the WHO Executive Board meeting in January, where Member States plan to discuss building on the successes of this past year by fully implementing and financing the programme’s new strategy. Rotary and other key global GPEI partners are planning a renewed and intensified outreach across the broader international development community to secure the necessary financial resources to achieve success. Polio immunization campaigns will also continue in full force in both endemic and outbreak countries.
Twelve months ago, the programme was in a much different place, as WHO and UNICEF launched an Emergency Call to Action to draw attention to the need for renewed commitment. A year later, thanks to a strengthened and unified response, the GPEI is meeting the moment and is more committed than ever to end all forms of poliovirus, once and for all.
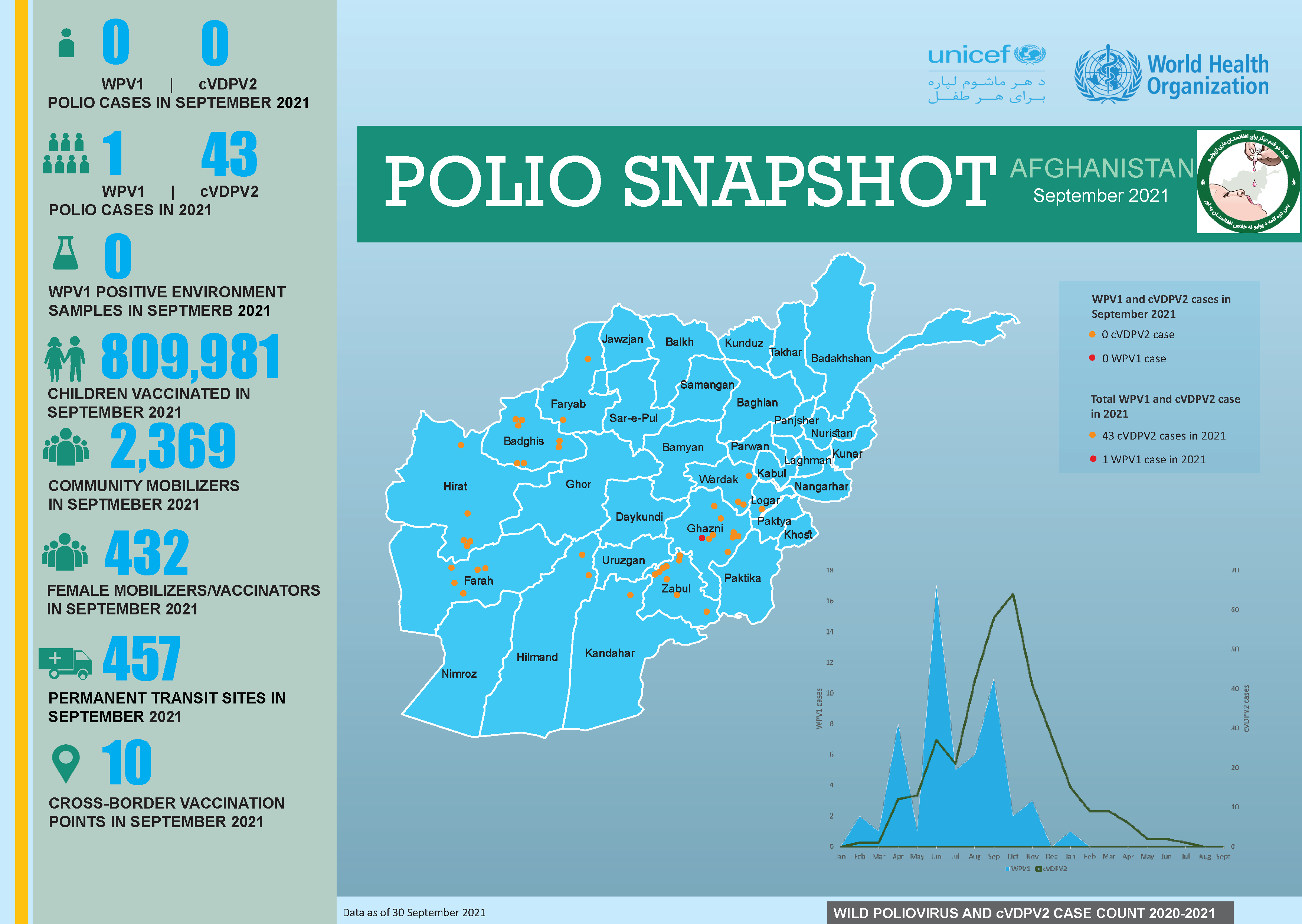
In September:
No new Wild Poliovirus (WPV1) case and no new cVDPV2 cases were confirmed.
25 August 2021 – “Poliovirus circulation does not stop during conflicts, it does not stop during emergencies. If anything, it makes children and families even more vulnerable by adding a layer of risk”, says a Polio Provincial Officer from Balkh province.
Despite risks and challenges due to the recent insecurity, the polio programme is staying and delivering for the children of Afghanistan. Our 315 staff and more than 70,000 polio health workers across the country remain firm in their resolve to eradicate polio. Their work ensures that critical polio activities continue while adapting to the rapidly changing situation and carry on even when hostility levels are high.
In 2021, one wild poliovirus type 1 (WPV1) and 43 circulating vaccine-derived poliovirus type 2 (cVDPV2) cases have been confirmed in Afghanistan. All cases have been reported in areas of the country that have for years been inaccessible for door-to-door vaccination campaigns, which left at least 3 million children repeatedly deprived of polio vaccination. Population displacement brought about by the current situation could further impact the programme’s access to children and increase immunity gaps against polio, triggering a rise in transmission. It is also feared that the mixing and movement of unvaccinated populations due to the upheaval faced by thousands of Afghans may spur polio transmission.
“We are working with all actors, to ensure there are no delays or disruptions to polio vaccination campaigns and overall routine immunization. Gains of the past twenty years cannot be lost. Children need immunization now, they must not bear the brunt of conflict and instability. We are calling for unimpeded access to all children,” says Dr. Dapeng Luo, WHO Representative in Afghanistan.
Pre-planning and resilience measures
While the current situation is a challenge, it is by no means the first the polio programme has faced. Using its wealth of knowledge from many years of operating in complex environments, the programme has invested in robust, pre-emptive contingency planning to be able to adapt and continue delivering. Regular monitoring of the security situation has allowed for nimble decision making.
The programme has moved swiftly to ensure safety and security of its staff. Its international staff footprint has been significantly reduced and vulnerable national staff and their dependants have been temporarily relocated to Kabul. Flexible working arrangements and salary advances have been provided to cover urgent needs of staff and polio health workers, who are the backbone of polio operations.
Around eighty percent of polio staff remain at their field locations and working to maintain essential polio services, supported remotely by colleagues who have needed to relocate.
“I am filled with pride for my team and their strong resolve, courage and passion. They are the heroes children of Afghanistan need right now. Thanks to their efforts, Acute Flaccid Paralysis (AFP) and environmental surveillance never stopped. Except for a few locations that experienced temporary disruptions last week, stool sample collection, visits to active health facilities, case investigation, the shipment of samples to Pakistan for laboratory testing, and the collection and transport of sewage samples for polio environmental surveillance remain unaffected. COVID-19 surveillance, which the polio programme has been supporting since last year, has also continued,” says Irfan Elahi Akbar, Polio Team Leader, WHO Afghanistan.
Polio vaccinations are continuing through permanent transit teams in most regions and at cross-border sites, including Friendship Gate (between Afghanistan and Pakistan).
After a brief pause, the National Emergency Operation Center is back up-and-running and undertaking planning needed to implement future campaigns. Discussions are ongoing with local authorities to safeguard the resumption of critical immunization activities across the country. The programme remains optimistic that polio vaccination campaigns planned for later this year can go ahead, however, is maintaining a flexible approach.
“The safety and security of staff and polio health workers is our top priority. Their commitment to ending polio is nothing short of inspirational. I stand ready to support their critical work in any way I can. I say this with absolute conviction: We will achieve a polio-free world,” said Dr. Hamid Jafari, Director of Polio Eradication, WHO Eastern Mediterranean Region.
The Global Polio Eradication Initiative (GPEI) is closely monitoring developments in Afghanistan. GPEI partners and staff are currently assessing immediate disruptions to polio eradication efforts and the delivery of other essential health services, to ensure continuity of surveillance and immunization activities while prioritizing the safety and security of staff and frontline health workers in the country.
The polio programme in Afghanistan has operated for many years amid insecurity and conflict, and will continue working with all actors, agencies and organizations who enable delivery of immunization as well as deliver humanitarian assistance to populations in need across the country. The GPEI remains steadfastly committed to protecting all children from polio and supporting the provision of other essential immunizations and health services.
We strongly believe that the delivery of health care – including polio vaccination – is essential to prevent diseases and safeguard communities. Together with our partners, the people of Afghanistan, national and provincial authorities, we will do everything in our power to continue this critical work.
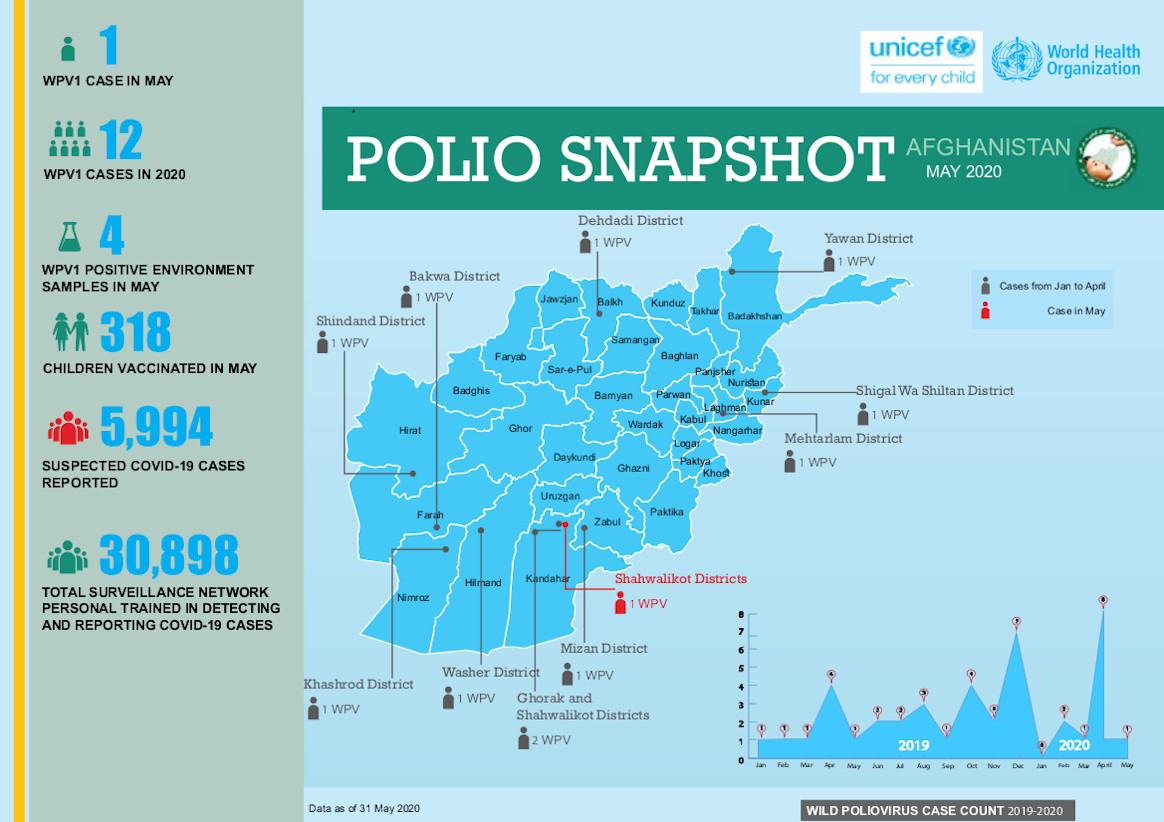
In May:
No new Wild Poliovirus (WPV1)cases and 5 new cVDPV2 cases were confirmed.
Meeting virtually this week at the 74th World Health Assembly (WHA), global health leaders and ministers of health noted the new Global Polio Eradication Initiative Strategic Plan 2022-2026 and highlighted the importance of collective action to achieve success.
Member States emphasised the urgency of implementation of the strategic plan and urged the WHO Secretariat and Member States to build on recent advances to keep surveillance high, ensure sustained, improved coverage in campaigns and respond rapidly to outbreaks. Several Members States welcomed the establishment of a new EMRO Ministerial Regional Subcommittee on Polio Eradication and Outbreaks, and roll-out of the novel oral polio vaccine type 2 (nOPV2) to more effectively and sustainably address outbreaks of circulating vaccine-derived polioviruses (cVDPVs). The Minister of Health of Egypt, Dr Hala Zaid, as a Co-Chair of the Regional Sub-Committee said: “The Regional Subcommittee offers a new, ministerial-level channel to galvanize political support, leverage funding, particularly domestic funding, and raise the profile of polio as a Public Health Emergency of International Concern. Its establishment reflects the firm commitment of the Eastern Mediterranean Region to do whatever it takes to stamp out poliovirus transmission and achieve eradication.”
Dr Ahmed Al-Mandhari, the Regional Director for the Eastern Mediterranean, addressed the delegates and noted a year of hard work across the Region. He emphasised the critical step of establishing the ministerial Sub-Committee to ensure more coordinated support for the remaining wild poliovirus-endemic and polio outbreak-affected countries in the Region. Speaking of the new vaccine, Dr Al-Mandhari said, “We are also at the dawn of what we hope will be a new era in responding to VDPV type-2 outbreaks, with an improved vaccine, the novel oral poliovirus type 2, approved for Emergency Use Listing and soon to be used in the Region.”
Member States noted support for local community, progress on closing outbreaks and welcomed efforts to unite with other initiatives to close gaps in immunization. The WHA paid tribute to female frontline workers and highlighted their role in building community relationships. Amid the new COVID-19 reality, the WHA also expressed deep appreciation for the GPEI’s ongoing support to COVID-19 response. WHO’s Deputy Director-General, Dr Zsuzsanna Jakab, highlighted the value of the polio infrastructure in addressing public health emergences, noting that the polio network has been the first in line of defence for COVID-19 response in many countries, and now providing valuable support to the rollout of Covid-19 vaccines. “It is our chance to retain the polio knowledge and expertise to build back stronger and more robust health systems. If we don’t act now, we will lose this enormous opportunity,” said Dr Jakab.
The Regional Director for the African Region, Dr Matshidiso Moeti, thanked African countries and partners for rapidly restarting and innovating to deliver polio activities after a pause during the COVID-19 pandemic, especially following the successful certification of eradication of wild polioviruses last year in the region. Integrating polio functions into other programmes will be critical to maximising the gains against this disease, she said, and to leveraging the wealth of expertise and experience that has been built.
Rotary International welcomed the new strategy and its priority on integration and extended collaboration with partners, as well as its focus on gender equality. Gavi, the Vaccine Alliance, highlighted the new strategy’s alignment with the Immunization Agenda 2030 and Gavi’s new 5-year strategy, and shared importance of reaching 0-dose children and missed communities with comprehensive and equitable immunization services.
Aidan O’Leary, WHO Director for Polio Eradication, addressed delegates, saying: “Wild poliovirus transmission is restricted to Afghanistan and Pakistan, and while we have seen a sharp decrease in incidence this year, this is no time for complacency. Gaining and sustaining access to all children in Afghanistan and increasing coverage of missed children in core reservoir areas of Pakistan remain the key challenges, and we must all work together to overcome these to achieve and sustain zero cases. At the same time, we must continue to respond to cVDPV2s. The solutions focus not just on the new nOPV2, but also more timely detection, more timely and higher quality outbreak response and strengthening essential immunization services in zero-dose communities and children, aligned with the IA2030 agenda. The new strategy addresses the broader needs of communities through expanded integration and partnership efforts along six distinct workstreams. Implementation will be strengthened through a more systematic approach to performance, risk management and accountability at all levels.”
The new strategy – Delivering on a Promise – will be officially launched at a virtual event on 10 June 2021. Details about the event are available here.
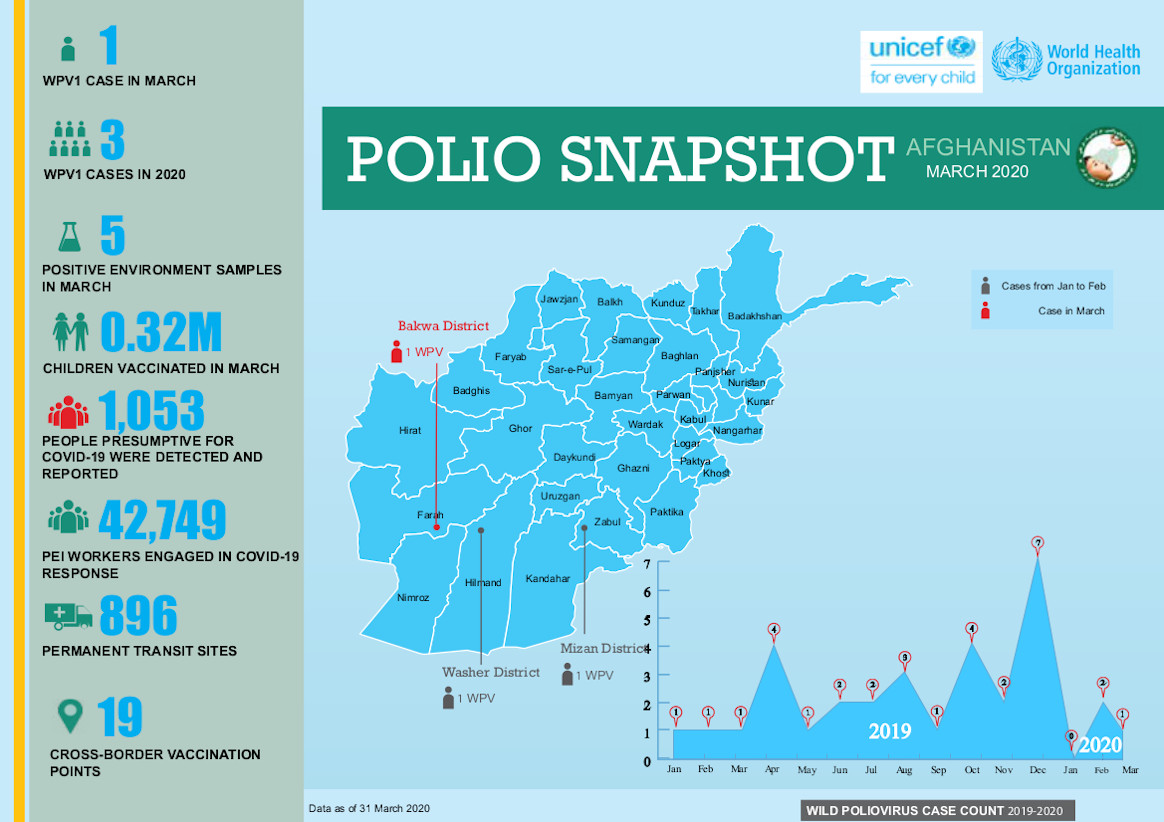
In March:
No case of WPV1 was confirmed
6,649,243 children were vaccinated against polio during the March National Immunisation Days (NIDs)
The new Regional Subcommittee brings together ministers of health from Member States across the Eastern Mediterranean Region to tackle some of the persistent high-level challenges to polio eradication. Those include raising the visibility of polio eradication as a regional public health emergency and priority and mustering the political support and domestic financial support needed to finish the job.
During the inaugural meeting convened by the Regional Director, Dr Ahmed Al-Mandhari, two co-chairs were elected to drive the regional push: Egypt’s Minister of Health and Population, H.E Dr Hala Zayed, and the Minister of Health and Prevention of the United Arab Emirates, H.E. Abdul Rahman Mohammed Al Oweis.
H.E. Abdul Rahman Mohammed Al Oweis was represented at the meeting by Dr Hussain Al Rand, the Assistant Undersecretary for Health Centres and Clinics and Public Health, United Arab Emirates. Both Member States flagged the urgency of the state of polio transmission in the last polio-endemic region at present, but also the opportunity to leverage greater regional coordination to achieve eradication.
Polio eradicators around the world know that ours is, in many ways, a grassroots programme: we use microplans to work through neighbourhoods door to door, household to household. But big-picture solidarity is needed to maximize the success of our ground-level efforts.
Wild poliovirus transmission has spread beyond core reservoirs of polio endemic Afghanistan and Pakistan, infecting 140 children in 2020. Outbreaks of circulating vaccine-derived poliovirus type 1 (cVDPV1) paralysed 29 children in Yemen. Type 2 outbreaks spread across the Region in 2020, paralysing 308 children in Afghanistan, 135 in Pakistan, 58 in Sudan and 14 in Somalia. At a time like this, moving forward as a region and as blocs, rather than on a country-by-country basis, is critical.
One of the issues identified by Member States as critical to stopping transmission is the movement of people across borders, and ensuring that surveillance and vaccination efforts target the increasing number of people who regularly cross borders across the region – whether they are moving as a consequence of conflict, environmental crises or economic necessity.
Interventions were made by Afghanistan, Egypt, the Islamic Republic of Iran, Iraq, Oman, Pakistan, Saudi Arabia and the United Arab Emirates. All statements reaffirmed strong support for the establishment of the subcommittee under the Regional Committee Resolution on polio eradication adopted in 2020.
Members of the subcommittee were unanimous in their commitment to engage in coordinated action and support of regional polio eradication efforts in four strategic areas. These include raising the visibility of the polio emergency in the Region, pushing for collective public health action, strengthening efforts to transition polio assets and infrastructure and advocating for the mobilization of national and international funding to achieve and sustain polio eradication.
A theme that ran through all Member States’ interventions was the idea of maximizing the resources already in place – including the workers, the polio and EPI infrastructure a across the region, and the array of community leadership groups with which the polio programme has worked in past.
“Last year or the year before the year before there was a meeting in Muscat with religious leaders from different countries, and I think we need to capitalize on their support. We need to give them ownership,” said Dr Ahmed Al Saidi, Minister of Health, Oman.
The COVID-19 pandemic has had an outsized impact on polio programmes across the region. The four-month pause in vaccination, from March-July 2020, gave the virus a window to spread almost unchecked. While we are immensely proud to have shouldered much of the COVID response burden, with GPEI infrastructure still supporting that response, this has come at a cost: nearly 80 million vaccination opportunities were lost.
“But we are moving forward, making up lost ground and, through this new Regional Subcommittee, leveraging the credibility that the polio programme has built through its pivot to COVID-19 and back again to polio,” said Dr Hamid Jafari, Director of the regional polio programme and co-facilitator of the Regional Subcommittee.
That credibility is now the polio’s most valuable asset: the proof that polio programmes are not just a means to battle polio, but sophisticated, fast-moving public health assets skilled in pandemic response.
The subcommittee will report its progress to WHO’s governing bodies meetings, including the World Health Assembly and the Regional Committee for the Eastern Mediterranean.
The Secretariat, which is made up of the office of the Regional Director and members of the regional polio eradication programme from WHO’s Eastern Mediterranean Region, will support the subcommittee to develop a programme of work based on the key outputs of the group.
Anisa’s story epitomizes the heroic contribution of women polio workers in Afghanistan who continue building trust in vaccines among parents and caregivers in the quest to immunize every last child and end polio.
The yellow taxi drives slowly on an unpaved Afghan road. It has rained heavily turning the detritus on the ground into a muddy quagmire, and the car labours in its efforts not to get stuck.
Stopping near a house, a young woman in a black scarf and traditional dress climbs out of the car. This woman is Anisa, a UNICEF consultant for the polio programme. Today she is visiting parents who are refusing to let their children be vaccinated, to explain why the two drops of oral polio vaccine (OPV) are critical for their health and wellbeing.
We enter one of the houses and meet an elderly woman.
“I am not vaccinating my grandchildren!” The woman sounds resolute, but we stay anyway. “Can we talk about something else?” Anisa asks calmly. Shortly thereafter, we’re drinking tea and praising the mild weather. The grandmother tells us her left leg was almost fully paralyzed half a year ago and she can’t walk normally.
“This is horrible. You should go to the clinic. I can recommend a good doctor for you. And do you also know that children who are not immunized can also be paralysed because of polio?” Anisa starts getting to the point of our visit. “You have two wonderful granddaughters and it’s easy to protect them.”
The grandmother doesn’t seem convinced but asks questions about the rumours around the vaccine. Anisa explains that OPV is safe, halal for Muslims, and it is the only way to protect children from getting polio. One hour later, the grandmother nods – she finally agreed to vaccinate. It is hard to say what was the turning point that convinced her. Maybe the photos of paralyzed polio survivors that Anisa showed her on her phone; maybe information that polio vaccination is required for Hajj and Umrah (religious pilgrimages to Mecca which must be done at least once in lifetime by all Muslims); or simply the fact that Anisa vaccinated her own two children, and they are safe and well. The fact that the grandmother finally agreed to vaccination feels like a big victory – but it’s just a small step in the battle against polio.
Anisa has been working in the health sector for almost 10 years – as a midwife, female mobiliser vaccinator, nutrition officer and a clinical mentor. She first started to support the polio programme as a Provincial Communication Officer (PCO), supervising over a hundred communication cluster supervisors.
During the national immunization campaigns, even during the COVID-19 pandemic, Anisa supports the teams by conducting information sessions for refusal families and arranging discussion sessions for community groups. She also holds awareness raising sessions on how to prevent the spread of COVID-19.
“After my first day working with refusal families, I wanted to leave the job. I didn’t convince anyone. But then I managed to convince one family with five children, who have never been vaccinated and it felt like such a victory that I decided to stay,” remembers Anisa. “Now I know how to approach different people; I understand what type of information is important to persuade them to make the right decision.”
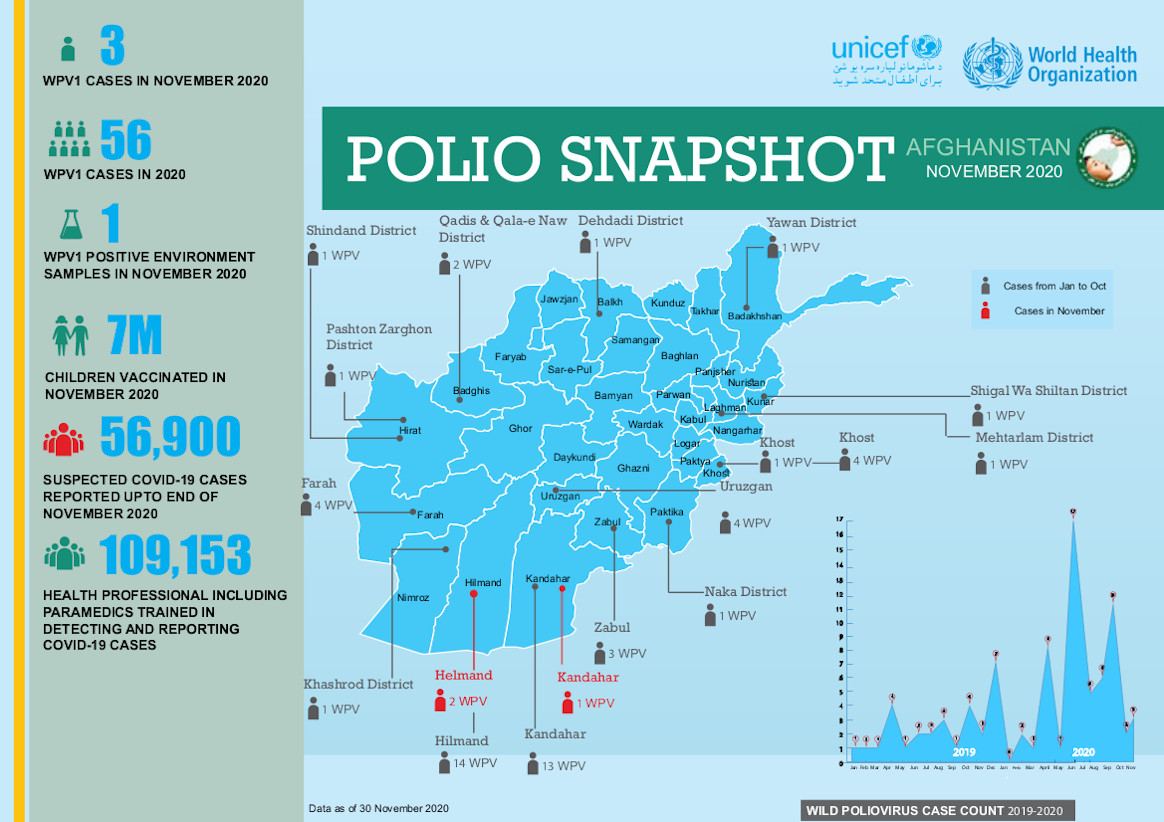
In November:
3 cases of Wild Polio Virus (WPV1) were confirmed
54 cross-border teams and 288 permanent transit teams (PTTs) were operational across Afghanistan in November 2020.
These teams vaccinated 79,489 and 538,674 children, respectively.
On a wintery November day, vaccinators across Afghanistan wrapped up warm, checked that they had facemasks and hand sanitizer, and headed out into the cold morning. Their mission? To reach 9.9 million children with polio vaccines, before snowfall blocked their way.
From valleys to muddy lanes, we look at some of the environments where vaccinators work, as well as some of the key challenges that have made 2020 one of the toughest years for polio eradicators.
Panjshir province
For some vaccinators, the first snows had already arrived. At the top of the Panjshir valley, Ziaullah and Nawid Ahmad started their day at 7am.
“We walked six hours to Sar-e Tangi and back to take polio drops to the last houses in the valley”, said Ziaullah. The mountainous roads in this area are impassable by car, so vaccinators walk many kilometers to the most remote villages. Sar-e Tangi means ‘top narrow edge’, and the view during the long winter is of snowy peaks.
A few kilometers from Sar-e Tangi, father Arsalan Khan was proud to have protected his own and other children in the extended family with polio drops. He said, “I ensure all the children in the family are vaccinated during each round the drops were offered and of course I will keep vaccinating them each time the vaccinators visit our village”.
Khan continued, “The vaccinators walk long distances across the mountain slopes to our villages, sometimes during harsh weather conditions, to bring polio drops to our doors.”
“Thanks to the people and countries that support the vaccination campaigns and make it possible for the drops to reach our doorsteps.”
In Badakhstan, Mr. Azizullah had COVID-19 safety measures on his mind. Like all vaccinators working for the polio programme, he had been trained on how to safely deliver polio drops during the pandemic. The temperature was below zero, with the first snow on the ground, as Mr. Azizullah walked through the rugged terrain from home to home, ensuring to wear his mask and regularly sanitize his hands.
Mr. Abdul Basit and Misbahuddin, volunteers in nearby Aab Barik village said, “It is cold and walking through muddy lanes is not easy, but we have to do our job. There was one case of polio in Badakhshan so that means there is probably virus circulation and we have to stop that”.
Mr. Abdullah, a university lecturer observing vaccination activities in Herat, said, “I believe a vaccinator’s job is more important than mine. I really appreciate their work and appreciate the international community for making the polio immunization operations possible in Afghanistan with their financial support.”
“I believe that all these efforts will be fruitful, hopefully soon, and we will get rid of the virus in our country”.
The November campaign was particularly aimed at boosting the immunity of unvaccinated children, and children who have not received their full vaccine doses. Many children have missed out on polio vaccines and other routine immunizations due to a pause in vaccination activities in the first few months of the COVID-19 pandemic. Health workers are now racing against time to protect the youngest children from the poliovirus.
Ms. Sitara, mother of Yasameen, who was wrapped up warm against the elements, said, “I am very happy to be able to immunize my daughter and protect her against polio”.
In the east region of Afghanistan, 8,530 volunteers, 160 district coordinators and 786 cluster supervisors were hard at work, aiming to reach as many children as possible during the campaign.
Dr. Akram Hussain, Polio Eradication Initiative Team Lead for WHO in the region explained, “We were not able to do house to house campaigns in some parts of the region. As a result many children were missed during the October vaccination campaigns”.
Despite the best efforts of vaccinators, in October, 3.4 million children nationwide missed vaccines due to factors including insecurity, the COVID-19 pandemic and vaccine mistrust. The year 2020 has seen a significant rise in polio cases and detection of the virus in the environment, and the disease is present in almost all provinces.
The programme is aiming to reach more children and tackle virus spread next year. Activities include targeted campaigns in high risk districts, collaborating with the religious scholars from the Islamic Advisory Group to encourage vaccine uptake and communicating more effectively with communities.
The incredible contributions of the polio programme to COVID-19 response are testimony to the agility and adaptability of Afghanistan’s programme in the most difficult circumstances. Many hope that lessons learnt from this experience can be applied to achieving the eradication goal.
Ending polio requires everyone – including polio personnel, communities, parents, governments and stakeholders – to commit to overcoming challenges. As the weather turns colder and snow continues to fall, many are looking ahead to what 2021 holds for polio eradication in Afghanistan.
In a year marked by the global COVID-19 pandemic, global health leaders convening virtually at this week’s World Health Assembly called for continued urgent action on polio eradication. The Assembly congratulated the African region on reaching the public health milestone of certification as wild polio free, but highlighted the importance of global solidarity to achieve the goal of global eradication and certification.
Member States, including from polio-affected and high-risk countries, underscored the damage COVID-19 has caused to immunization systems around the world, leaving children at much more risk of preventable diseases such as polio. Delegates urged all stakeholders to follow WHO and UNICEF’s joint call for emergency action launched on 6 November to prioritise polio in national budgets as they rebuild their immunization systems in the wake of COVID-19, and the need to urgently mobilise an additional US$ 400 million for polio for emergency outbreak response over the next 14 months. In particular, Turkey and Vietnam have already responded to the call, mobilising additional resources and commitments to the effort.
The Assembly expressed appreciation at the GPEI’s ongoing and strategic efforts to maintain the programme amidst the ‘new reality’, in particular the support the polio infrastructure provides to COVID-19-response efforts. Many interventions underscored the critical role that polio staff and assets play in public health globally and underline the urgency of integrating these assets into the wider public health infrastructure.
At the same time, the GPEI’s work on gender was recognized, with thanks to the Foreign Ministers of Australia, Spain and the UK for their roles as Gender Champions for polio eradication.
Delegates expressed concern at the increase in circulating vaccine-derived poliovirus (cVDPV) outbreaks, and urged rapid roll-out of novel oral polio vaccine type 2 (nOPV2), a next-generation oral polio vaccine aimed at more effectively and sustainably addressing these outbreaks. This vaccine is anticipated to be initially rolled-out by January 2021.
Speaking on behalf of children worldwide, Rotary International – the civil society arm of the GPEI partnership – thanked the global health leaders for their continued dedication to polio eradication and public health, and appealed for intensified global action to address immunization coverage gaps, by prioritizing investment in robust immunization systems to prevent deadly and debilitating diseases such as polio and measles.
Dr Elaha, at 22 years old, is a medical graduate and a District Polio Officer. She’s also helping fight the COVID-19 pandemic in Afghanistan.
“COVID-19 has affected both our work life and personal life. When I joined the polio team, I had plans to take initiative and look for innovative ways to fight polio, however, with the COVID-19 pandemic all my plans were challenged,” she says. “Campaigns were postponed and the number of cases were on the rise.”
The temporary pause in polio vaccination campaigns, necessary to keep health workers and communities safe during the early months of the pandemic, led to a widened immunity gap in both Afghanistan and Pakistan, the only two countries that still harbour wild poliovirus. Now, polio teams are urgently working to close the gap while continuing their support to Afghanistan’s COVID-19 response. To ensure their safety, all polio personnel have been trained to take precautionary measures against COVID-19, including wearing masks correctly and regular handwashing.
Dr Elaha doesn’t underestimate the danger of her work to fight COVID-19. She explains, “I start my day at 8am by visiting private and public clinics, pharmacies, traditional healers at their homes. Of course, I am worried about myself and my family getting COVID-19. My mother is elderly, and COVID-19 can be dangerous for her.”
“However, I am committed to serve my people and go out in the field to help save others’ lives. It is not easy. My family understand that I am a medical doctor, so no matter what virus is there, I have to do my job as a doctor.”
Through her work, Dr Elaha has come up against rumours and misinformation. A major part of both ending polio and fighting COVID-19 is working to inform and build trust with communities about diseases and how they can be prevented.
Elaha says, “A lot of people thought that COVID-19 was a disease of nonbelievers. At first, when I used to go to clinics, because of my medical degree, they respectfully listened to me. However, when I talked about COVID-19 and washing hands and other preventative methods, they would tell me that this disease was for nonbelievers.”
“Unfortunately, a lot of people got sick and many also lost their lives. People have started to believe the pandemic. They know that people can get sick and die of the disease.”
Although public awareness about the dangers of COVID-19 has improved, Dr Elaha believes there is still plenty to do to encourage communities to adopt disease prevention measures such as widespread mask wearing.
Until the pandemic is over, she is determined to work long hours to fight both polio and COVID-19. The polio workforce currently contributing to COVID-19 response includes almost 36,000 members of the Polio Surveillance Network, and over 47,000 polio frontline workers.
“I chose to continue to do public health awareness during the COVID-19 pandemic. I wanted to help save people’s lives and continue to serve my people,” says Farida, a polio worker and volunteer for the COVID-19 response.
Seven months since the first COVID-19 case was reported in Afghanistan, female polio programme frontline workers continue to support outbreak response. Often, they put concerns for their health to one side as they work in areas with many COVID-19 cases. Sometimes, their work brings them into conflict with the social norms of their community and society.
Farida has been working with the polio programme since 2010. Starting as a volunteer, she has moved up the ranks to become a district polio officer.
During the pandemic, Farida has taken on extra duties to identify suspected COVID-19 cases, share accurate information and trace individuals returning from abroad to ensure they are isolating.
On a typical day she heads out to speak to small groups of women about hygiene, breastfeeding, nutrition and measures to prevent COVID-19. She is the focal point for communicable diseases within her clinic, and so must also keep all her colleagues up to date on the latest information about COVID-19, alongside reinforcing knowledge about polio and the importance of vaccination.
Farida’s work is often emotionally challenging. “Luckily, I still have not contracted COVID-19,” she says.
“I reported seven people as I suspected that they had COVID-19, unfortunately six of them died and one of them survived and is healthy now.”
Ever since the first case of COVID-19 was reported in Afghanistan, the Polio Eradication Initiative (PEI) programme has been supporting the government response.
Since March 2020, nearly 36,000 members of the Polio Surveillance Network, almost 44,000 polio frontline workers, about 95,000 health providers and about 5,000 government and NGO staff have been trained on COVID-19 surveillance. Over 178,000 community and religious influencers have been trained to deliver outreach messages, and almost 7,000 coordination meetings have been held.
About 10,000 COVID-19 and polio surveillance visits have been made to health facilities, and more than 2,500 medical facilities have been surveyed for COVID-19 preparedness. Thanks to the efforts of the polio team, over 46,000 cases of COVID-19 have been detected, of which more than 8,000 have been confirmed.
Farida shares with her colleagues a sense of duty to her fellow citizens. She says, “I go out hoping that my work might save lives. If I stay home, who will give the information to people that I do?”
Vaccinators in countries including Afghanistan, Angola, Burkina Faso and Pakistan took to the streets this month to fill urgent immunity gaps that have widened in the under-five population during a four month pause to polio campaigns due to COVID-19.
Campaigns resumed in alignment with strict COVID-19 prevention measures, including screening of vaccinators for symptoms of COVID-19, regular handwashing, provision of masks and a ‘no touch’ vaccination method to ensure that distance is maintained between the frontline worker and child. Only workers from local communities provided house-to-house vaccination to prevent introduction of SARS-CoV2 infection in non-infected areas.
Although necessary to protect both health workers and communities from COVID-19, the temporary pause in house-to-house campaigns, coupled with pandemic-related disruptions to routine immunization and other essential health services, has resulted in expanding transmission of poliovirus in communities worldwide. Modelling by the polio programme suggests a potentially devastating cost to eradication efforts if campaigns do not resume.
In Afghanistan, 7858 vaccinators aimed to vaccinate 1 101 740 children in three provinces. Vaccinators were trained on COVID-19 infection control and prevention measures and were equipped to answer parents’ questions about the pandemic. Through the campaign, teams distributed 500 000 posters and 380 000 flyers featuring COVID-19 prevention messages.
In Angola, 1 287 717 children under five years of age were reached by over 4000 vaccinators observing COVID-19 infection prevention and control measures. All health workers were trained on infection risk, and 90 000 masks and 23 000 hand sanitizers were distributed by the Ministry of Health.
In Burkina Faso, 174 304 children under five years of age were vaccinated in two high-risk districts by 2000 frontline workers. Vaccinators and health care workers were trained on maintaining physical distancing while conducting the vaccination. 41 250 masks and 200 litres of hand sanitizer were made available through the COVID-19 committee in the country to protect frontline workers and families during the campaign.
In Pakistan, almost 800 000 children under the age of five were reached by vaccinators in districts where there is an outbreak of circulating vaccine-derived poliovirus. Staff were trained on preventive measures to be followed during vaccination, including keeping physical distance inside homes and ensuring safe handling of a child while vaccinating and finger marking them.
“Our early stage analysis suggests that almost 80 million vaccination opportunities have been missed by children in our Region due to COVID-19, based on polio vaccination activities that had to be paused,” said Dr Hamid Jafari, Director for Polio Eradication in the Eastern Mediterranean Region. “That’s close to 60 million children who would have received important protection by vaccines against paralytic polio.”
Over the coming months, more countries plan to hold campaigns to close polio outbreaks and prevent further spread, when the local epidemiological situation permits.
“Our teams have been working across the Region to support the COVID-19 response since the beginning of the pandemic, as well as continuing with their work to eradicate polio,” said Dr Hamid Jafari. “We must now ensure that we work with communities to protect vulnerable children with vaccines, whilst ensuring strict safety and hygiene measures to prevent any further spread of COVID-19”.
Dr Matshidiso Moeti, WHO Regional Director for Africa, commented, “We cannot wait for the COVID-19 pandemic to be contained to resume immunization activities. If we stop immunization for too long, including for polio, vaccine-preventable diseases will have a detrimental effect on children’s health across the region.”
“The campaigns run by the Polio Eradication Programme demonstrate that mass immunization can be safely conducted under the strict implementation of COVID-19 infection prevention and control guidelines.”
In March 2020, polio social mobilisers from the UNICEF-run Immunization Communication Network (ICN) provided routine immunization referral services to over 37,000 children in southern and eastern Afghanistan.
The polio programme’s routine immunization efforts in Afghanistan have made important gains, especially in the country’s east, in the areas bordering Pakistan. Polio social mobilisers support mother and child health referral services, and help families keep track of their children’s health records. As the mobilisers are recruited from their community, they know the families in their neighborhood and can trace each child’s planned immunization schedule from birth.
It is critical that routine immunization continues throughout the pandemic to protect children from life-threatening diseases including polio. Polio mobilisers have found their work is even more valued during the COVID-19 response.
Masoud, a polio mobiliser, says ‘’I used to announce the immunization sessions through the Mosque but not all the targeted children were brought to the health facility. Now through the ICN support to routine immunization, the number of missed children has reduced due to tracking of every child in the community and coordinating with the health facility.”
“This is critical during the ongoing pandemic, as families are not sure if they can leave their homes to take their children to the health facility for immunization. The polio mobilisers are their guide in the community.’’
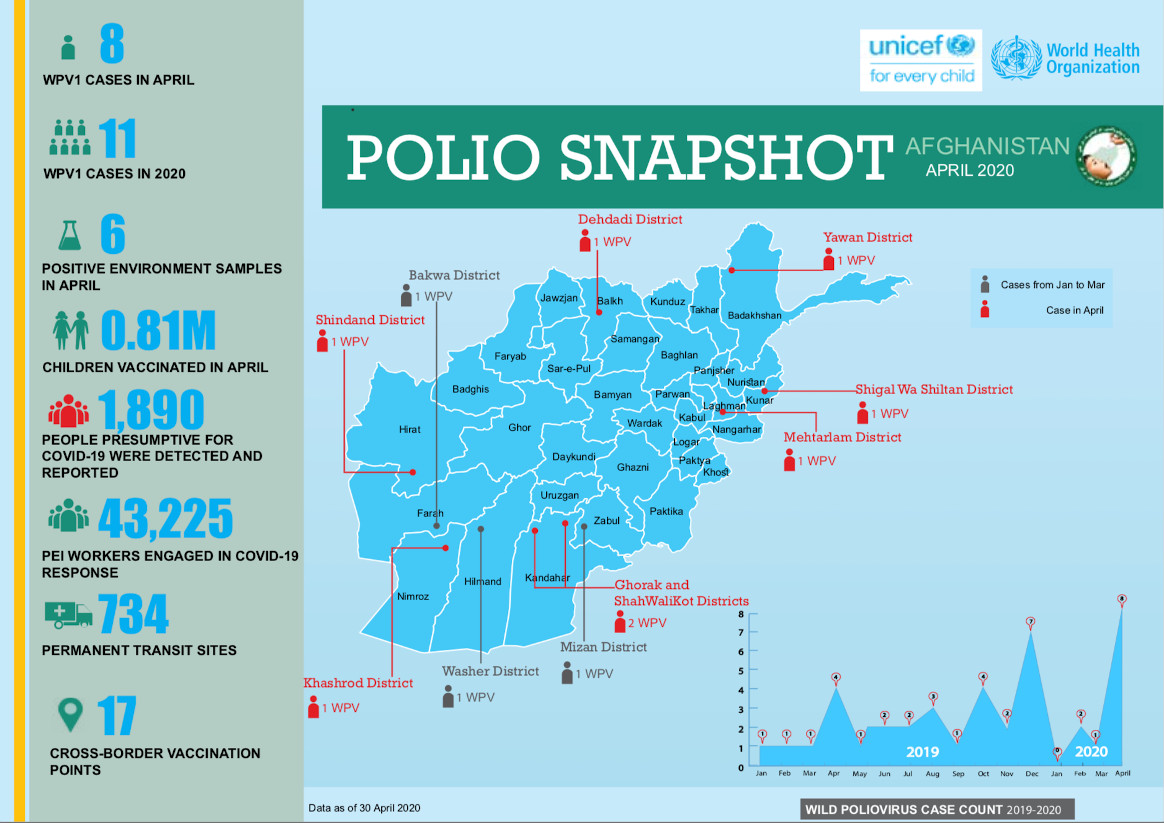
In April
8 cases of wild poliovirus were reported
0.81 million children were vaccinated.
Permanent transit teams vaccinated 776,818 children and cross-border teams vaccinated 33,609 children
In 2003, Melissa Corkum received a call that would change her life. The World Health Organization wanted to interview her for a position in their polio eradication team. Like most people who are hearing about polio eradication for the first time, the story compelled her, and she packed her bags to embark on a new adventure. Seventeen years later, she remains a dedicated champion of polio eradication.
A self-proclaimed ‘virus chaser’, Melissa has worked in all three polio endemic countries – Afghanistan, Pakistan and Nigeria. She found inspiration in her first field job in Nigeria, where she realized the scale of the polio eradication programme and that she was a part of something tremendous in public health history.
“I was amazed and inspired when I first saw the efforts of the front-line workers delivering vaccines to the doorstep. It may seem simple to deliver a couple drops into a child’s mouth, but when you see it in motion for the first time, it is truly remarkable,” Melissa said.
To this day, Melissa remains in awe of the work required to make ‘reaching every child’ possible. From mobilizing financial resources, to getting vaccines where they need to be while keeping them cool. From the microplanning to ensure all children and their houses are on a map, to the mobilization of champions in support of polio and immunization. Along the way, the stewards of these processes play an essential role to deliver the polio vaccine.
Melissa has worn many hats during her time in polio eradication, but her current role may be the most challenging yet. As the Polio Outbreak Response Senior Manager with UNICEF, she must answer the formidable challenge of containing outbreaks, using her expertise to inform global policy, strategy and operations.
To do this Melissa spent 80% of her time in the field prior to the outbreak of COVID-19, working with partners of the Global Polio Eradication Initiative (GPEI), Ministries of Health and local health workers.
Her work is a mix of challenge and excitement – the challenges of containing outbreaks, including those affected by the COVID-19 emergency – and excitement in developing new tools and methods to overcome the evolving challenges that present barriers to eradicating polio.
“There is never a dull day no matter what hat you may be wearing within this programme. If we are going to put an end to polio for good, we are going to have to fight the fight on a number of fronts – endemics and now the emerging issue of outbreaks in a post-COVID world,” said Melissa.
“The key is a willingness to do whatever it takes to get the job done.”
At times, Melissa felt the weight of the enormous challenges to eradicate polio, especially during her time in Afghanistan, where protracted conflict has complicated efforts to deliver basic services to the most vulnerable. Melissa often reflects on her time as Polio Team Lead there and the emotional rollercoaster she faced trying to stay ahead of the virus, while watching the tragedy of war unfold in the country.
“But when I felt down, I would pick myself up and get ready to face the next challenge. I found hope and inspiration in the resilience of the Afghan people, especially the women who worked in the polio programme, risking their lives and demonstrating a courage that stood out amidst all the difficulties.”
Melissa sees gender as one of the keys to polio eradication. She firmly believes that the only way to tighten the gaps in the system is by involving and empowering women equally in all roles across the programme, and that the only way to reach every child is to ensure their caregivers are equally informed and engaged in the decision making process.
“Unless we involve more women in the programme in certain corners of the world, we will continue to reach the same children and miss the same children, making polio eradication ever more difficult,” Melissa said.
“Change won’t happen if we don’t change the way we think about involving women. We need to listen to their views and open the doors for more women to join and participate equally from the community level and all the way to the leadership, decision-making level.”
Melissa was born in a small town in Nova Scotia, Canada. Her views on the critical involvement of women and gender equality in the polio programme very much align with her government’s Feminist Aid Policy. The Government of Canada has been a long-time champion of polio eradication and recently generously pledged C$ 190 million to assist the GPEI achieve its objectives of polio eradication.
Greater gender equity is one of the legacies that the polio programme is working to leave behind after eradication. Reflecting on her career, Melissa explains what keeps her working to defeat polio after all these years.
“It is so inspiring to be part of something tangible and something that is completely possible if we commit ourselves to doing everything possible to find every last child”.
In response to the COVID-19 pandemic, the polio programme has diverted thousands of personnel to fight the virus. Repurposing extensive experience eradicating polio, the programme is supporting country response in areas including information dissemination, disease surveillance, risk communications and data management.
Community social mobilizers stepped up in March to deliver soap bars and information on COVID-19 to some of Afghanistan’s poorest and most vulnerable communities.
Social mobilizers are local people trained to communicate with the public about specific health issues in ways that are understandable and encourage behaviours to protect health. In Afghanistan, UNICEF coordinates a network of 3,750 mobilizers.
Social mobilizer Feroz explained the importance of his mission. “The families were especially happy with the soap distribution. If the social mobilisers were not here, people would have remained uneducated about COVID-19.”
Just a few days after the decision to mobilize polio teams for COVID-19 response, Feroz’s team distributed thousands of soap bars and educational materials on the virus to communities across his province. Many of the families served have limited access to adequate sanitation products or facilities. Providing a bar of soap and demonstrating its use is a simple COVID-19 prevention measure.
During the distribution, the teams emphasized the importance of routine immunization continuing throughout the pandemic, reminding parents to take their children to health facilities. With house-to-house polio vaccination campaigns paused for the time being, many more children may be vulnerable to polio and other vaccine-preventable diseases if they do not receive vaccinations at health clinics.
The soap packaging carried a pro-vaccine message, reading ‘let’s come together for a polio-free Afghanistan.
Zuhal, a colleague of Feroz, explained that she has noticed a change in how vaccine hesitant families react to the polio social mobilisers since the beginning of COVID-19 pandemic. ‘’The number of people who were interested exceeded our expectations. We were able to attract our communities’ attention. Parents who used to refuse polio vaccine in campaigns have participated in COVID-19 discussions and eagerly asked for information.’’
She added, ‘’During the last polio campaign, I had to wait 30 minutes in front of one house. When the door was opened, a man told me, “Go, we do not want to vaccinate our children. Never come here again”. The same man looked for me in his neighbourhood during our COVID-19 information and soap distribution, and this time he was desperate for information. This shows that people in the community recognize that we are a source of information when they are concerned about their health, even if they have rejected polio vaccines in the past.’’
Feroz agreed, saying, “The community has more trust in us now we are trying to minimize the risk of COVID-19 infection through public education.’’
It is hoped that the trust built up between the mobilizers and communities during this time will translate into stronger relationships far into the future. This may help the polio programme reach out to children in families where vaccination has previously been viewed with suspicion.
Feroz is pleased to serve his community. He says, “I feel proud seeing the results of my work, when children receive routine immunization on time and pregnant women deliver safely at the hospital. Knowledge matters.”
He adds, “Information at the time of crises can be lifesaving. The polio programme has a mission to protect every child against diseases – polio and now COVID-19.”