RIYADH (28 APRIL 2024) – Today, at the first-ever World Economic Forum (WEF) Special Meeting hosted in Riyadh, the Kingdom of Saudi Arabia has pledged US$ 500 million over the next five years to support the work of the Global Polio Eradication Initiative (GPEI).
This announcement marks a significant increase in funding for the global effort to eradicate polio – a devastating virus that paralyzes and can be fatal for children but is preventable with vaccines. The funds announced today will enable GPEI partners – the Bill & Melinda Gates Foundation (BMGF), Gavi, the Vaccine Alliance, Rotary International, the United Nations Children’s Fund (UNICEF), the U.S. Centers for Disease Control and Prevention (CDC), and the World Health Organization (WHO) – spearheaded by national governments, to protect more than 370 million children with polio vaccines every year. It will also facilitate the delivery of other life-saving interventions like nutritional supplements and bed nets to underserved communities and strengthen health systems to better prepare countries for emerging health threats.
The commitment was made as part of a broader more than US$ 620 million partnership by Saudi Arabia and BMGF to support polio eradication and contribute to other global health initiatives, including the Lives and Livelihood Fund. The partnership was announced at the WEF Special Meeting by His Excellency Dr. Abdullah A. Al Rabeeah, Advisor to the Royal Court and Supervisor General of the King Salman Humanitarian Aid & Relief Centre (KSrelief) and His Excellency Fahad bin Abdurrahman Al-Jalajel, Minister of Health of the Kingdom of Saudi Arabia, in the presence of Dr. Tedros Adhanom Ghebreyesus, Director-General of the WHO, and Bill Gates, co-chair of BMGF.
H.E. Dr. Abdullah A. Al Rabeeah commented, “In Afghanistan and Pakistan, the last remaining polio-endemic countries, we have seen significant progress, yet work remains to be done as the world pushes towards making eradication possible. The pledge from Saudi Arabia today will enhance the innovation and collaboration needed to eradicate this disease. Together with our partners, the Bill & Melinda Gates Foundation, the Global Polio Eradication Initiative, the Islamic Development Bank and key countries across the region, our support will not only aim to end polio but to also strengthen health systems in these countries.”
“This investment towards global health isn’t just a good to have; it’s a strategic imperative for a thriving, more resilient future together,” said H.E. Fahad bin Abdurrahman Al-Jalajel, “the world faces many health challenges, and it is part of our responsibility and leadership to contribute with our partners in bridging the gaps, and through concerted efforts, we will be able to alleviate the suffering of many people.”
Thanks to decades of country leadership and global collaboration in delivering life-saving vaccines to billions of children, wild polio cases have fallen by 99.9% since the GPEI was founded in 1988 under the leadership of the World Health Assembly. More than 20 million people are walking today who would have otherwise been paralyzed by the virus. Just four cases of wild poliovirus have been recorded this year and 12 cases recorded last year in the remaining wild polio endemic countries of Pakistan and Afghanistan.
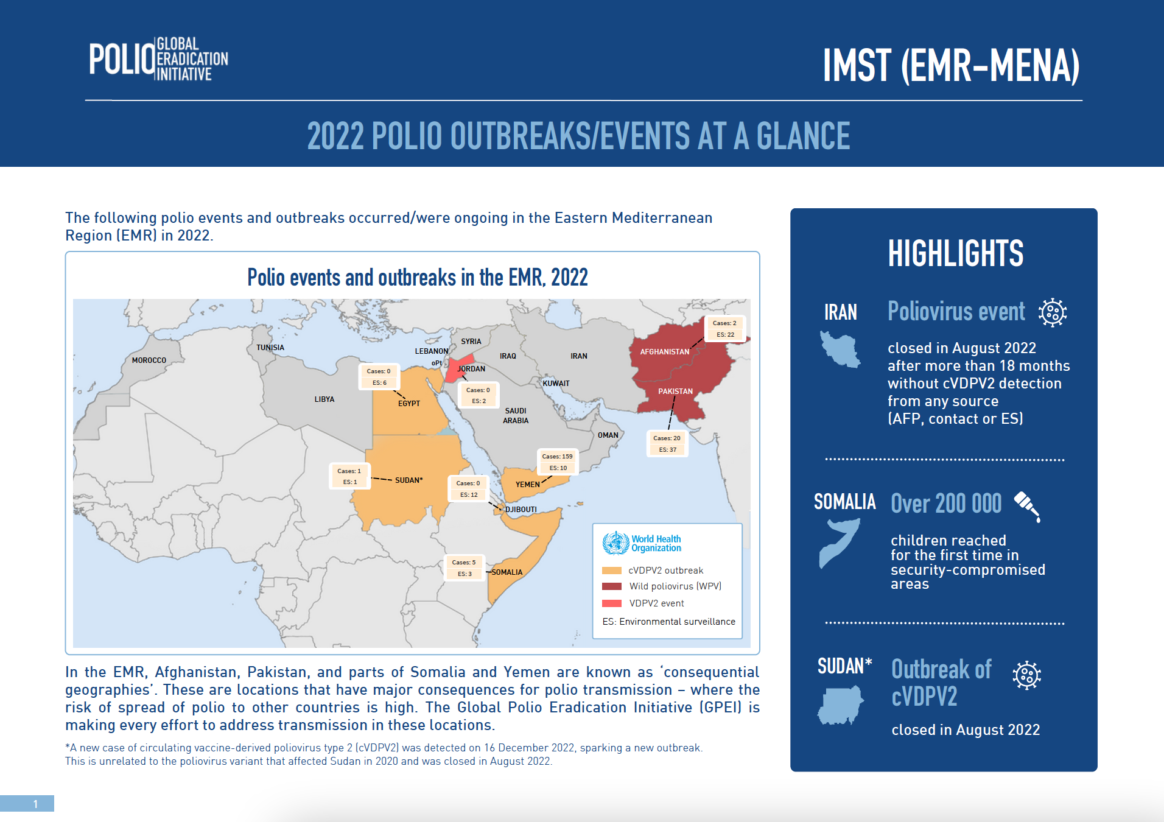
Meanwhile, outbreaks of variant poliovirus, which can emerge in places where not enough children are vaccinated against polio, are increasingly confined to high-risk areas in just four countries – Nigeria, the Democratic Republic of the Congo, Somalia, and Yemen. Still, in places where polio remains today, there are serious challenges to reaching all children with polio vaccines and other life-saving interventions, including vaccine misinformation, political insecurity, environmental disasters, and broader humanitarian crises.
“For decades, polio inflicted lifelong suffering on children and families. Today, we take another step toward finally eradicating it, thanks to the generous contributions of the Kingdom of Saudi Arabia. When we invest in eradicating polio, we make immunization and health systems more resilient, we equip nations to better respond to public health challenges, and most importantly, we ensure that more children will be able to live healthy lives,” said Bill Gates.
The announcement builds on a long history of support from Saudi Arabia and regional partners to the global polio eradication effort as well as across the Eastern Mediterranean – the last region where wild polio is endemic. For more than two decades, Saudi Arabia has not only financially supported the GPEI, but has also advocated for polio eradication and access to other life-saving vaccines in the Eastern Mediterranean and beyond. This support ranges from championing the cause among communities and religious leaders to advocating within major global convenings like the G20 and regional forums like the World Health Organization’s Eastern Mediterranean Regional Subcommittee for Polio Eradication and Outbreaks.
“Reaching all children with lifesaving vaccines is critical to ending polio and protecting children and communities everywhere from other preventable diseases and emerging health threats,” said Dr. Tedros Adhanom Ghebreyesus. “With this new funding, Saudi Arabia will help to protect children in even the hardest-to-reach areas, and move towards a healthier, polio-free world.”
“This important support will help bring us one step closer to eradicating polio once and for all,” said Catherine Russell, UNICEF Executive Director. “Together with communities, health workers, global partners, and donors like Saudi Arabia, we can help ensure that no child suffers from paralysis or dies from polio, and that more children have access to better health systems.”
To strengthen Afghanistan’s health systems and encourage a continued focus on achieving polio eradication in one of the world’s last polio-endemic countries, Saudi Arabia and the Gates Foundation have pledged US$ 3 million and US$ 15 million respectively over three years to support the Polio Legacy Challenge. This Challenge is a results-based financing initiative spearheaded by ministers of health in the region, including Saudi Arabia, the United Arab Emirates (UAE), and Qatar, under the auspices of the WHO EMRO Regional Subcommittee on Polio Eradication and Outbreaks.
Also today, as the Islamic Development Bank (IsDB) celebrates its 50th anniversary, Saudi Arabia announced US$ 100 million in new funding to support the IsDB’s Lives and Livelihoods Fund (LLF), which aims to lift the poorest out of poverty across 33 IsDB member countries through investments in primary health care, eliminating preventable infectious diseases like polio, supporting smallholder farming and rural agriculture, and improving basic infrastructure. This follows the UAE’s renewed pledge of US $50 million to the LLF announced earlier this week, continuing its support for the largest development fund in the region, which aids millions in low-income communities.
On the occasion, IsDB President Dr. Muhammad Al Jasser stated: “The Islamic Development Bank warmly welcomes the Kingdom of Saudi Arabia’s generous contribution to the Global Polio Eradication Initiative. This vital support strengthens GPEI’s efforts to eliminate this devastating disease. We’re proud that IsDB and ISFD, our poverty alleviation arm, have been among the top financiers for Pakistan’s polio eradication efforts, providing over US$ 555 million since 2012.”
“We also applaud the Kingdom of Saudi Arabia’s new funding for the Lives and Livelihoods Fund. This innovative initiative tackles poverty barriers faced by families, communities, and entire countries. We express our sincere gratitude to all partners, existing and new, for their continued collaboration and commitment. Together, through these concerted efforts, we can achieve the critical last-mile results needed to create a truly polio-free world,” added the IsDB President.
Additional quotes on the funding announcement:
Mike McGovern, Chair of the International PolioPlus Committee at Rotary International, said: “I extend heartfelt gratitude to Saudi Arabia for their commitment to the cause of polio eradication, which has been instrumental in advancing our collective mission towards a polio-free world. Together, we’ve witnessed the remarkable resilience of the polio eradication program, proving that with full support and collaboration, we can overcome any obstacle in our path. Let us continue to stand united in our efforts until polio is eradicated, ensuring a healthier, safer future for generations to come.”
Dr. Sania Nishtar, CEO of Gavi, the Vaccine Alliance, said: “This new commitment from the Kingdom of Saudi Arabia will not only help us achieve a polio-free world, it will help countries build stronger health systems, protecting families, communities and economies from other existing and emerging health threats.”
About the Global Polio Eradication Initiative
The Global Polio Eradication Initiative is a public-private partnership, spearheaded by national governments, WHO, Rotary International, the US Centers for Disease Control and Prevention, UNICEF, the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance. Since its launch in 1988, this partnership has helped prevent more than 20 million cases of paralysis, prevented more than 1.5 million childhood deaths and reduced the incidence of wild poliovirus by 99.9 percent, from more than 350,000 cases in more than 125 endemic countries, to twelve cases in two endemic countries in 2023.
Media Contact: Ally Rogers, Global Health Strategies (arogers@globalhealthstrategies.com)
About Islamic Development Bank (IsDB) Group
Rated AAA by the major rating agencies of the world, the Islamic Development Bank is the premier multilateral development bank of the Global South that has been working for 50 years to improve the lives of the communities it serves by delivering impact at scale. The Bank brings together 57 Member Countries across four continents, touching the lives of nearly 1 in 5 of the world population. Its mission is to equip people to drive their own economic and social progress at scale, putting the infrastructure in place enabling them to fulfil their potential. Headquartered in Jeddah, Kingdom of Saudi Arabia, IsDB has regional hubs and centers of excellence in 11 of its Member Countries. Over the years, the Bank has evolved from a single entity into a group comprising five entities: Islamic Development Bank (IsDB), the Islamic Development Bank Institute (IsDBI) tasked with research and training, the Islamic Corporation for the Insurance of Investment and Export Credit (ICIEC), the Islamic Corporation for the Development of the Private Sector (ICD), and the International Islamic Trade Finance Corporation (ITFC).