Even in face of global COVID-19 pandemic, governments and partners start the battle afresh, determined to finish polio once and for all
In a special one-off interview, PolioNews (PN) talks to both Aidan O’Leary (A-O’L) and Michel Zaffran (MZ) about the future of polio eradica...
New director joins with wealth of emergencies and public health experience
Plea for international solidarity, following WHO/UNICEF call for emergency action
Wherever she is in the world, Dr Gerber aims to deliver demonstrable impact to communities.
Dr. Tunji Funsho was honored as one of TIME's 100 most influential people for 2020.
Support from national governments and global donors critical to the region’s success against wild polio and must continue to achieve a polio...
Visit the "Africa Kicks Out Wild Polio" website for content on the WHO African Region’s efforts to eradicate wild polio.
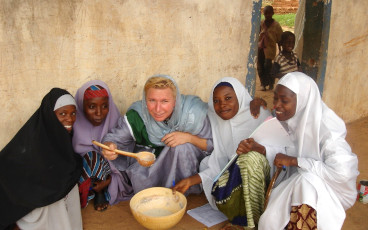
Meet a few of the women in Rotary playing a pivotal role in the effort to eradicate the disease
Polio social mobilisers have adapted their work to support families in Afghanistan.
Continued funding is crucial to respond to COVID-19, end polio and tackle other vaccine-preventable diseases.
Aziz Memon, incoming Rotary Foundation Trustee, explains why he’s determined to finish the task of polio eradication.
Countries and partners announce commitments to vaccinate 450 million children against polio each year and to overcome barriers to reaching e...
Part two in our series on the ‘plus’ in PolioPlus.
In the run up to the GPEI Pledging Event in November, the G20 Okayama Declaration emphasizes ending polio and delivering vaccines to all.
DG calls for doubling of efforts to now finish all remaining poliovirus strains
Global eradication of wild poliovirus type 3 declared on World Polio Day
The Polio Eradication Initiative is looking for innovative ways to detect, control and respond to anti-vaccination propaganda on social medi...
A series on the ‘plus’ in PolioPlus: preventing other diseases
UAE, partners, and donors in attendance as Global Polio Eradication Initiative introduces 2019-2023 Investment Case
Grassroots efforts got Nigeria over the barriers to polio vaccination
What drives our conviction? Have a read…
A unique look at immunization efforts in a sprawling water community
Political will apparent for Universal Health Coverage, Primary Health Care and polio eradication with Japan’s leadership
Research underway on a newer tool to protect children from polio and sustain a polio-free world