All travellers crossing the border between Pakistan and Afghanistan are vaccinated against polio, regardless of age
Polio programme assessed by experts at the global immunization meeting
Update on polio eradication efforts in Afghanistan for February 2019
JICA continues to support Pakistan in polio eradication efforts
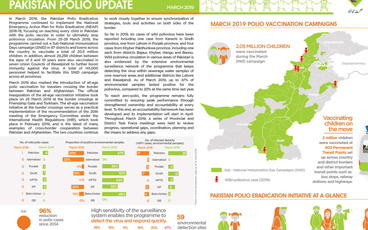
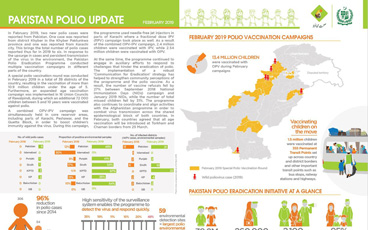
Update on polio eradication efforts in Pakistan for February 2019
Resilience and resolve are the keywords for women eradicating polio
Polio is a crippling disease still endemic in Afghanistan. However, the country is closer than ever to stopping transmission.
On International Women’s Day, we celebrate the role of women in the polio eradication efforts in Pakistan
Women health workers and have been highly effective in polio eradication efforts, often as the only point of contact in rural settings.
Surveillance officer at WHO pushes through gender-related obstacles to help end polio in Pakistan
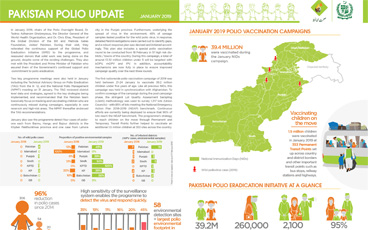
Update on polio eradication efforts in Pakistan for January 2019
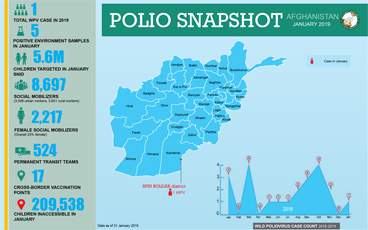
Update on polio eradication efforts in Afghanistan for January 2019
On the road to polio eradication in Pakistan.
New action plan to close gaps in polio detection
WHO Executive Board’s strong push to finish the job
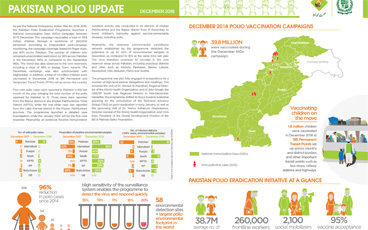
Update on polio eradication efforts in Pakistan for December 2018
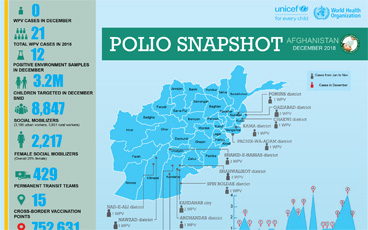
Update on polio eradication efforts in Afghanistan for December 2018
Progress in the challenging last mile of eradication
As the Global Polio Eradication Initiative (GPEI) enters its 31st year, the Chairs of the effort’s main global advisory bodies issue an extr...
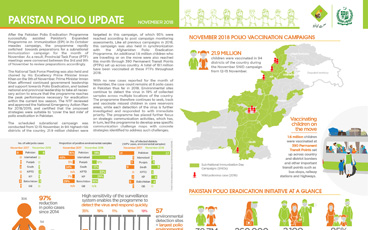
Update on polio eradication efforts in Pakistan for November 2018
Endemic countries, WHO and partners are committed to eradicate polio
Jean-Marc Olivé, Chairman of the Technical Advisory Group, reflects on what needs to be done to end polio in the Horn of Africa.
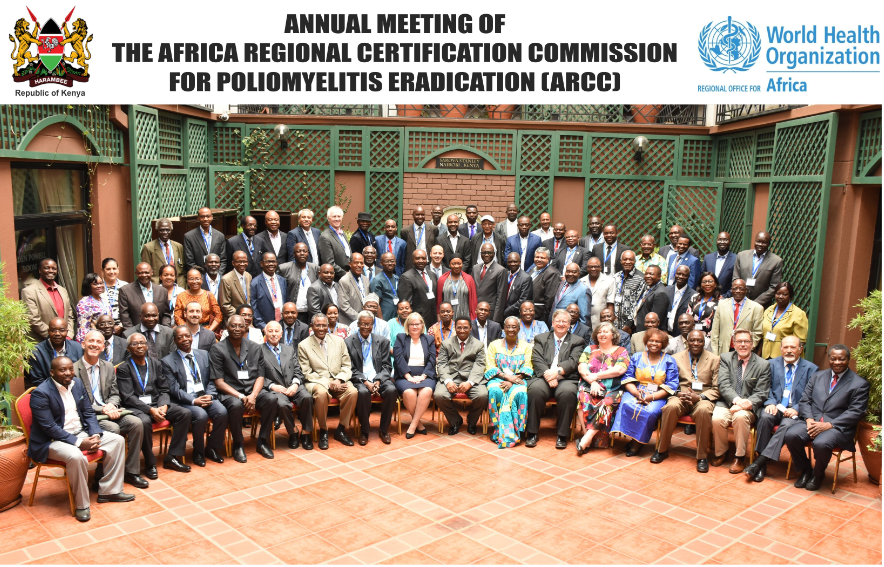
A review committee met in Nairobi to assess progress of the African region towards being certified polio-free
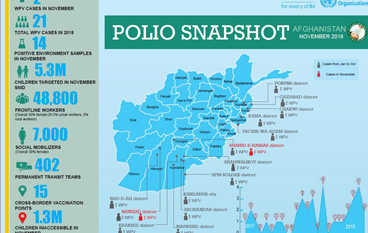
Update on polio eradication efforts in Afghanistan for November 2018