Joint statement from WHO and UNICEF
After a thorough evaluation, an independent Polio Outbreak Response Assessment Team (OBRA), has concluded that there is no evidence of ongoi...
New guidance anticipated to quicken progress in achieving necessary safeguards
Meeting in Berlin focused on supporting vaccine equity and pandemic response in developing countries
18 May 2022
Wild poliovirus type 1 detected in Lilongwe, Malawi
To prevent a possible outbreak, WHO and national health authorities have been implementing vaccination campaigns and boosting disease survei...
Ensuring nomadic children receive their polio vaccines is a formidable task.
GPEI head Michel Zaffran sheds light on the global cVDPV2 situation, the need for type 2-containing OPV, and implications for containment
Eastern Mediterranean Regional Commission for Certification of Poliomyelitis Eradication weighs in
Polio programme assessed by experts at the global immunization meeting
New action plan to close gaps in polio detection
Progress in the challenging last mile of eradication
As the Global Polio Eradication Initiative (GPEI) enters its 31st year, the Chairs of the effort’s main global advisory bodies issue an extr...
In the Horn of Africa polio outbreak, immunization efforts are focusing on a group known as “special populations”.
Early analysis of campaign data points to a successful vaccination round in a polio-free country at risk of possible importation.
Mohamed Shire, a polio eradication expert from Somalia, speaks about lessons from a life tirelessly working to eradicate first smallpox, the...
Papua New Guinea’s first polio case in decades is a champion for eradication
We speak to Dr Arlene King, Chair of the RCC for the Americas, and GCC Containment Working Group, about the vital importance of safe and sec...
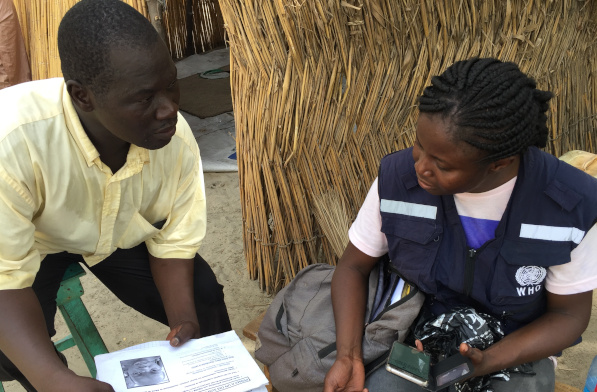
Across the Lake Chad Basin, e-Surve technology is revolutionizing the way that the polio programme conducts disease surveillance
Honorine Mollard Billard, Polio Eradication Officer at WHO, speaks to us about critical country support to vaccination campaigns in Lao PDR...
In the sahel surrounding Lake Chad, health workers provide vaccines to refugees and internally displaced people.
Flexible support to Nigeria also approved.