Vaccines alone do not end polio. Trust does. Access does. Showing up with more than one reason to open the door, does. That’s how Every Last...
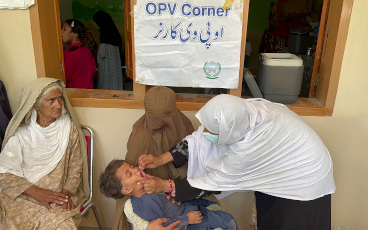
The preventive vaccination campaign led by Pakistan in partnership with the World Health Organization protected 34 million children against...
World Immunization Week highlights the importance of immunization globally
As of January 2024, Iraq has achieved the polio transition process in full. It is the first country among the polio transition priority coun...
Interviews with four experts
A new investment case shows that successful polio transition in the 8 priority countries of the WHO Eastern Mediterranean Region will have a...
To help end all polio transmission and meet the broader health needs of communities now, the GPEI works with a range of partners to integrat...
Global Polio Partners, Paris Saint-Germain Endowment Fund, and the French Gaming Community Unite to #ENDPOLIO
21 November 2023
Engaging digital communities to build trust in vaccines and eradicate polio
Country experiences show that success on polio transition is context specific.
How the polio program came together to help flood-affected frontline workers
21 March 2023
This report describes the initiatives implemented by four CSOs supported by the UN Foundation to enhance polio transition and integration ef...
“Rarely have I seen such commitment and dedication as I have seen in Pakistan.”
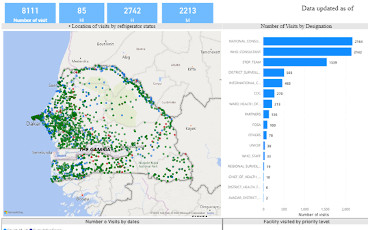
WHO Geographic Information System (GIS) equips over 200 specialists across Africa with essential digital mapping and Mobile Health skills to...
Teams urgently mobilized to help respond to disaster
New report provides evidence on role of polio workforce in COVID-19 vaccine rollout and essential immunization, and makes the case to sustai...
Statement
US$4.8 billion budget needed to implement new Strategy and eradicate the infectious disease Germany announces it will co-host polio pledgin...
The support polio teams provide to deliver COVID-19 vaccines underlines the vital role they can play for health priorities beyond polio.
07 September 2021