Update on polio eradication efforts in Pakistan for July 2019
Vaccination and religious dialogue
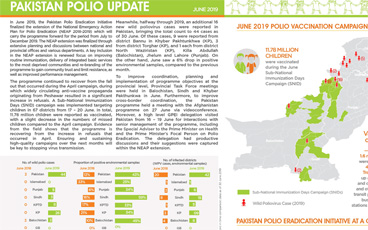
Update on polio eradication efforts in Pakistan for June 2019
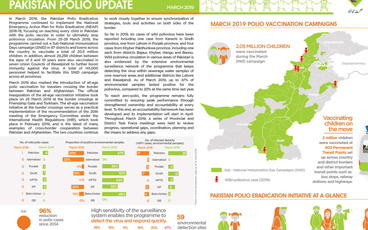
Update on polio eradication efforts in Pakistan for May 2019
Everyday people in Pakistan advocating for vaccinations
Update on polio eradication efforts in Pakistan for April 2019
Papua and West Papua provinces rise to challenges of stopping polio
Women are ensuring that the children in Papua New Guinea are protected and vaccinated
All travellers crossing the border between Pakistan and Afghanistan are vaccinated against polio, regardless of age
Update on polio eradication efforts in Afghanistan for February 2019
South Sudan leverages Smart Interactive visualization of Disease surveillance and Routine Immunization assessments
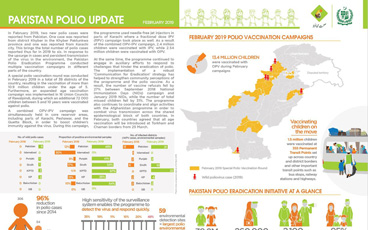
Update on polio eradication efforts in Pakistan for February 2019
Resilience and resolve are the keywords for women eradicating polio
With no wild poliovirus reported anywhere in Africa since 2016, efforts are being intensified to actively look for the virus, to ensure it i...
On International Women’s Day, we celebrate the role of women in the polio eradication efforts in Pakistan
Women health workers and have been highly effective in polio eradication efforts, often as the only point of contact in rural settings.
A look at some of the women in Somalia’s polio programme
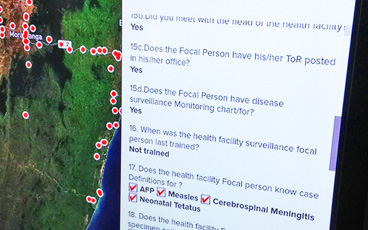
Surveillance officer at WHO pushes through gender-related obstacles to help end polio in Pakistan
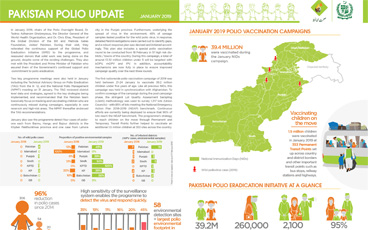
Update on polio eradication efforts in Pakistan for January 2019
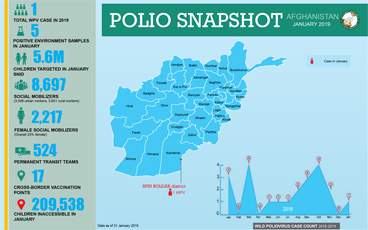
Update on polio eradication efforts in Afghanistan for January 2019
On the road to polio eradication in Pakistan.
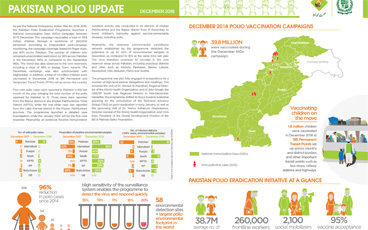
Update on polio eradication efforts in Pakistan for December 2018
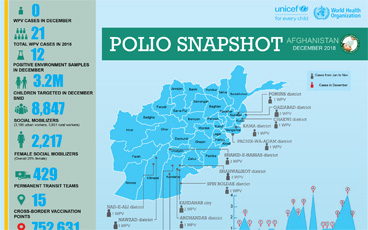
Update on polio eradication efforts in Afghanistan for December 2018
Progress in the challenging last mile of eradication