Over 140 public health experts from 22 countries gather at the 6th Regional Meeting on Polio in Guatemala
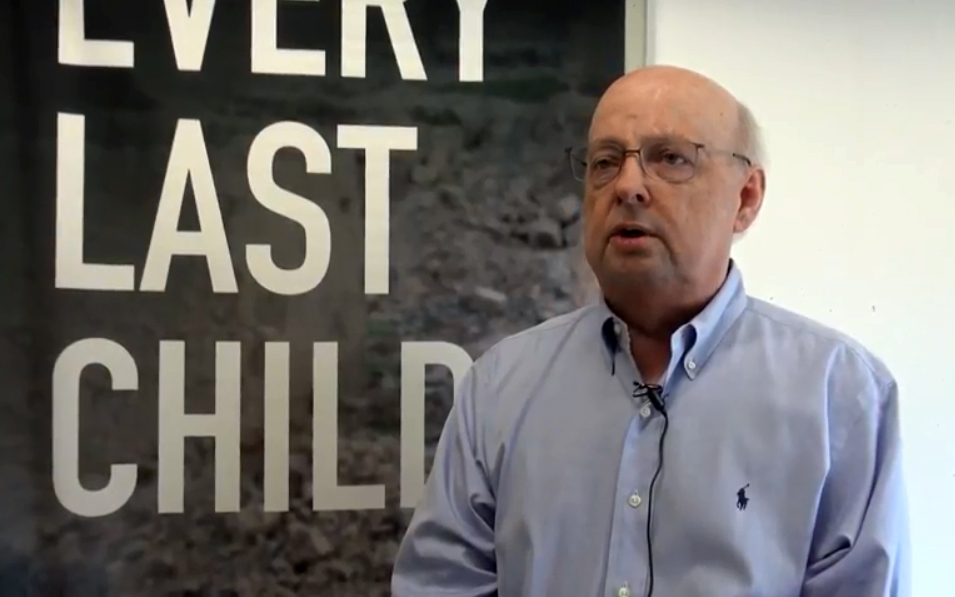
Jean-Marc Olivé, Chairman of the Technical Advisory Group, reflects on what needs to be done to end polio in the Horn of Africa.
A review committee met in Nairobi to assess progress of the African region towards being certified polio-free
We speak to Dr Arlene King, Chair of the RCC for the Americas, and GCC Containment Working Group, about the vital importance of safe and sec...
The last man with smallpox was an advocate for polio eradication.
“We reconfirm our resolve to work with partners to eradicate polio and effectively manage the post-polio transition.”
Polio discussions at this year’s World Health Assembly
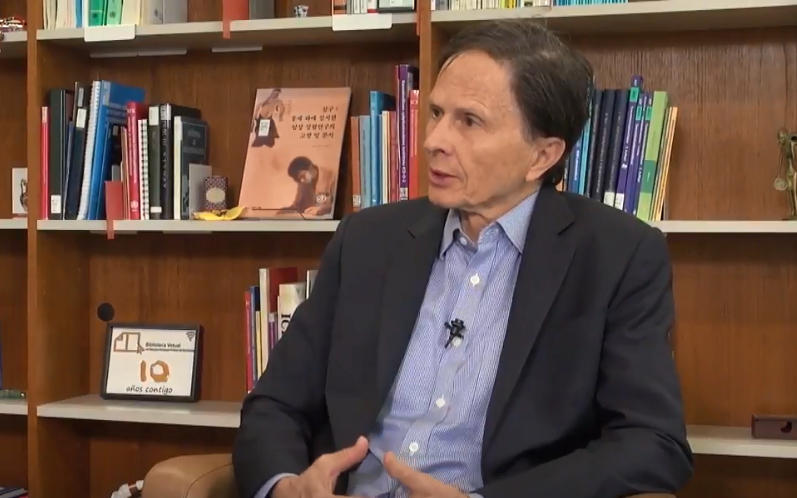
David Heymann, long-time public health expert, discusses what lessons smallpox eradication teaches us in eradicating a disease, and why it i...
Sweden is the first country to formally engage in the global poliovirus containment process
The global intensification of efforts to appropriately contain polioviruses is critical.
Towards a polio-free Africa: A chat with Professor Rose Leke, Chair of the African Regional Certification Commission.
We join Dr Urs Herzog, Rotarian, polio eradicator, National PolioPlus Advocacy Advisor for Rotary Switzerland and polio survivor himself, as...
Professor David Salisbury, chair of the Global Commission for the Certification of the Eradication of Poliomyelitis, talks us through the pr...