In January, children in Raqqa city received polio vaccines for the first time in two years as families return to the devastated city.
A week in the life of Auta, a vaccine facilitator in Borno State
La Dre Adele Daleke Lisi Aluma s’efforce d’atteindre les enfants jamais vaccinés
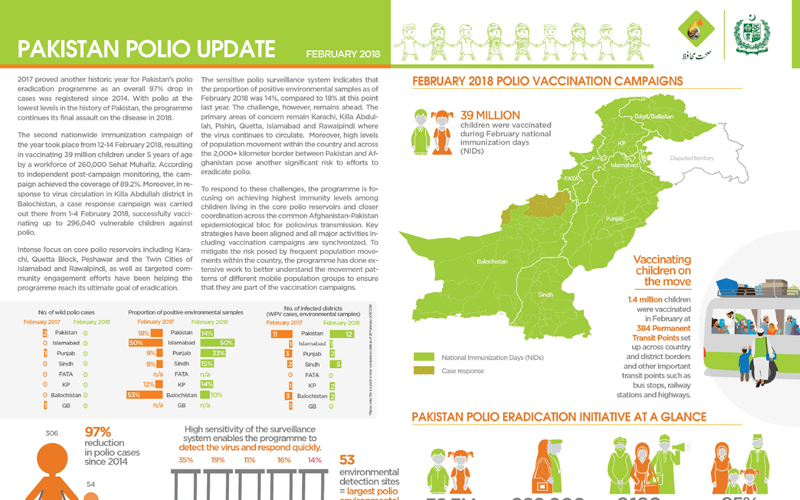
Update on polio eradication efforts in Pakistan for February 2018
What does it take to vaccinate every child in Afghanistan?
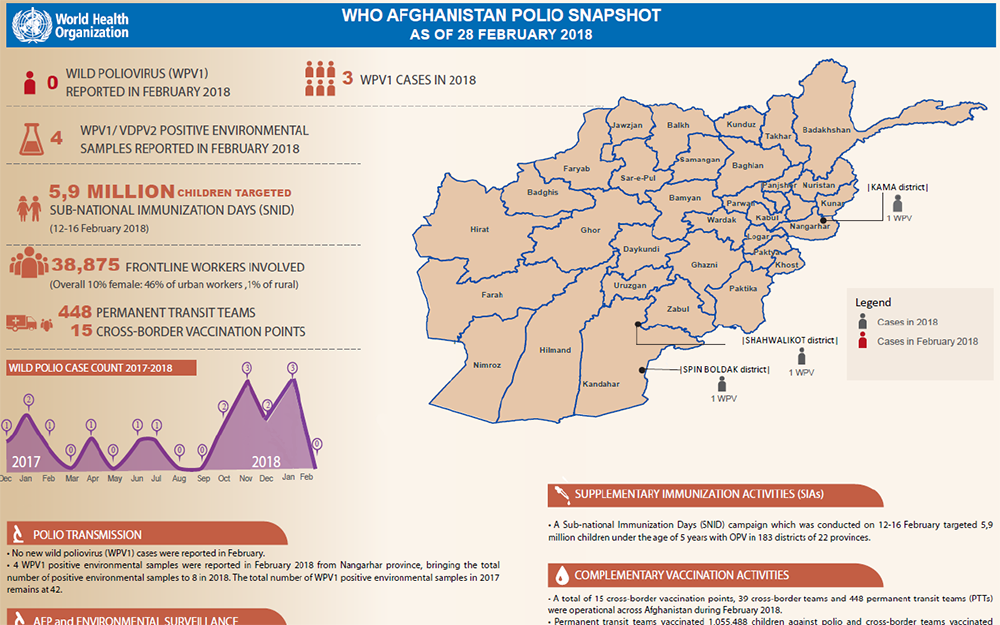
Update on polio eradication efforts in Afghanistan for February 2018
In Somalia, determined women are the face of polio eradication.
Dr Adele Daleke Lisi Aluma works to reach children who have never been vaccinated
In eastern Afghanistan, one family is helping to vaccinate every last child in their community
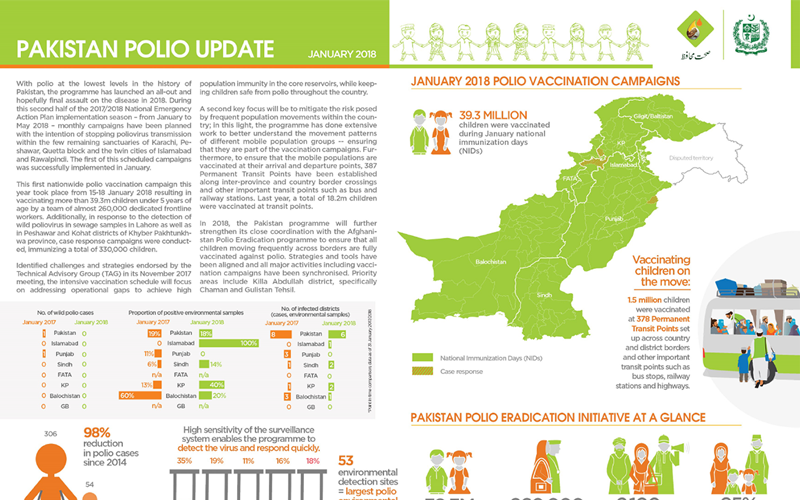
Update on polio eradication efforts in Pakistan for January 2018
In at-risk areas of Chad, large-scale polio campaigns are increasing the immunity of every child.
The strong polio eradication infrastructure in Borno is supporting Nigeria to vaccinate over eight million people against yellow fever.
In Afghanistan, frontline health workers explain to parents why the polio vaccine must be delivered multiple times
Polio can’t be cured, but it can be prevented. Two important tools help to prevent polio – two safe, effective vaccines. Find out about the...
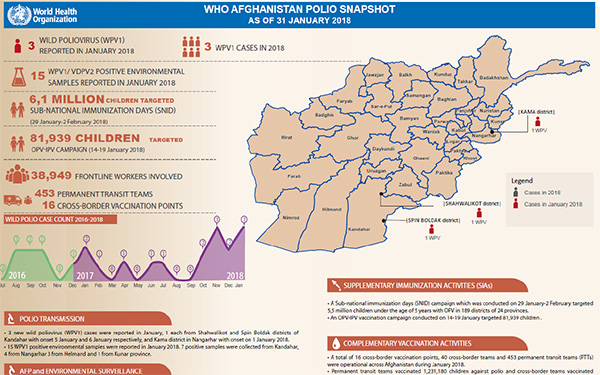
Update on polio eradication efforts in Afghanistan for January 2018
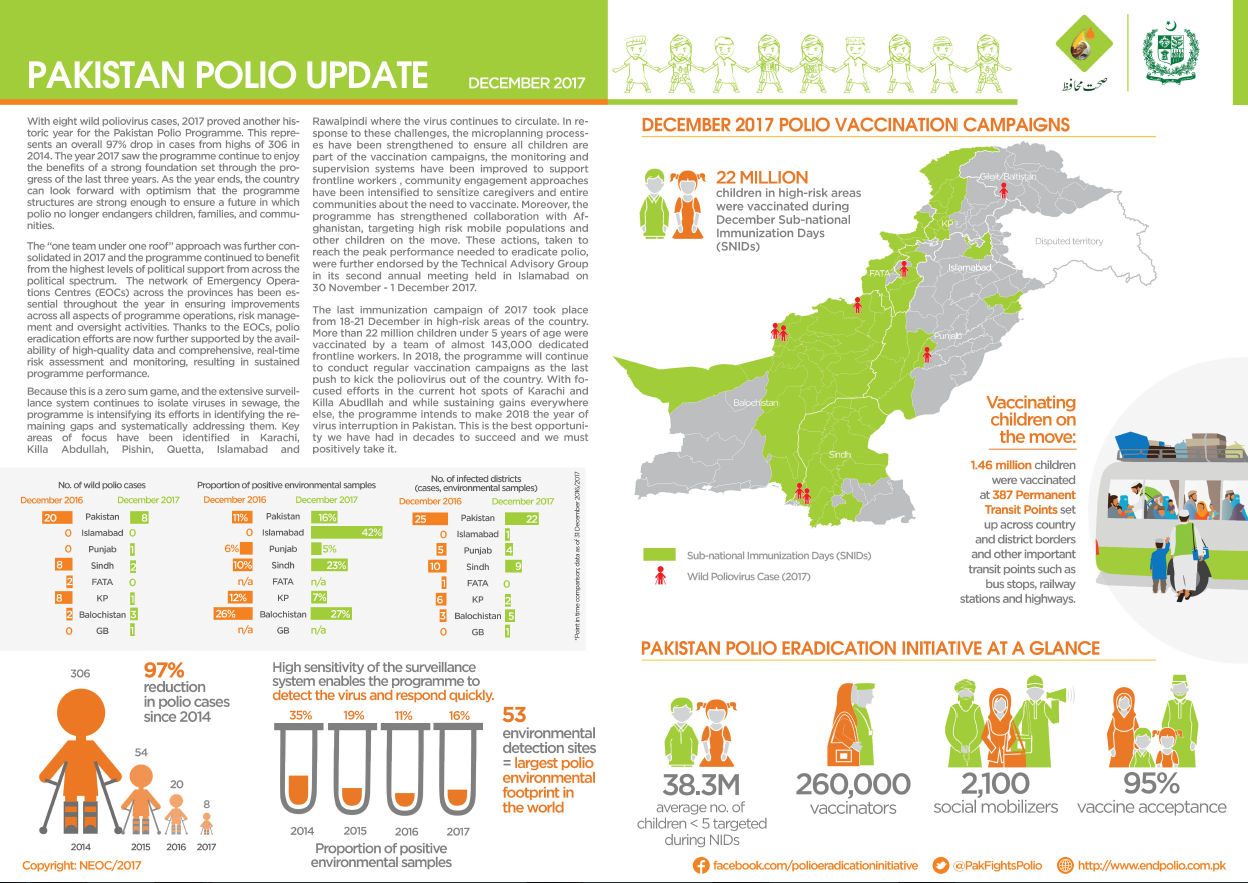
Update on polio eradication efforts in Pakistan for December 2017
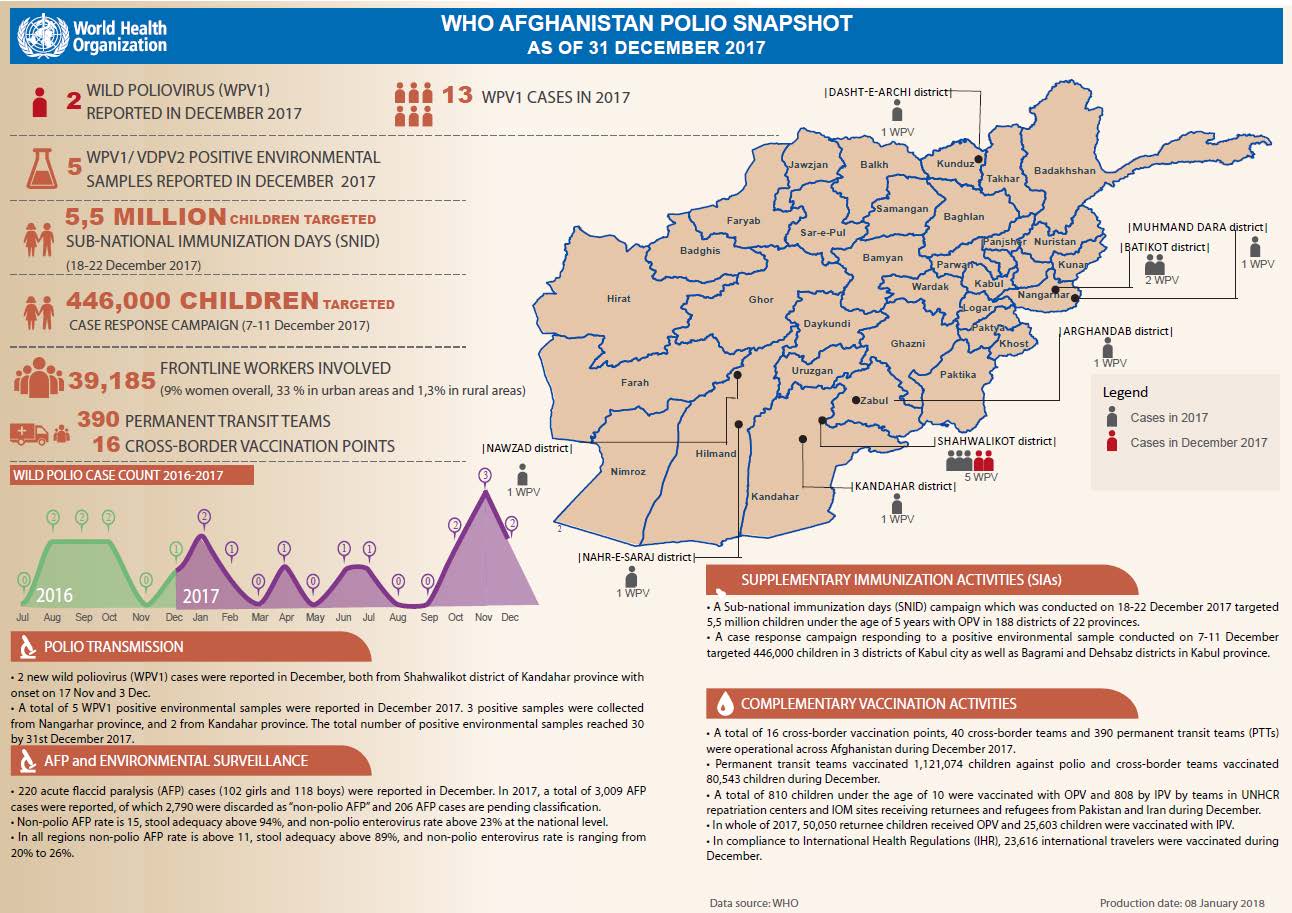
Update on polio eradication efforts in Afghanistan for December 2017
We join Dr Urs Herzog, Rotarian, polio eradicator, National PolioPlus Advocacy Advisor for Rotary Switzerland and polio survivor himself, as...
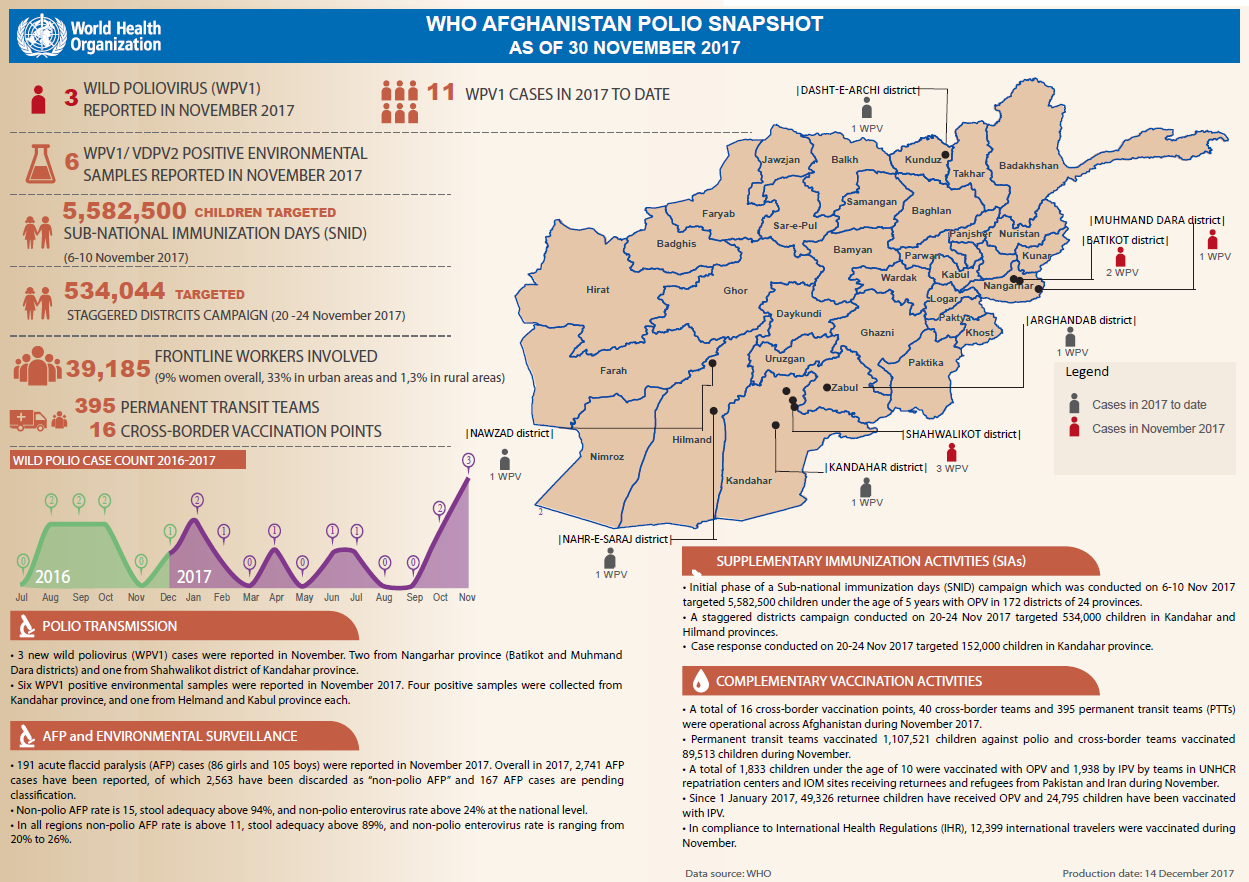
Update on polio eradication efforts in Afghanistan for November 2017
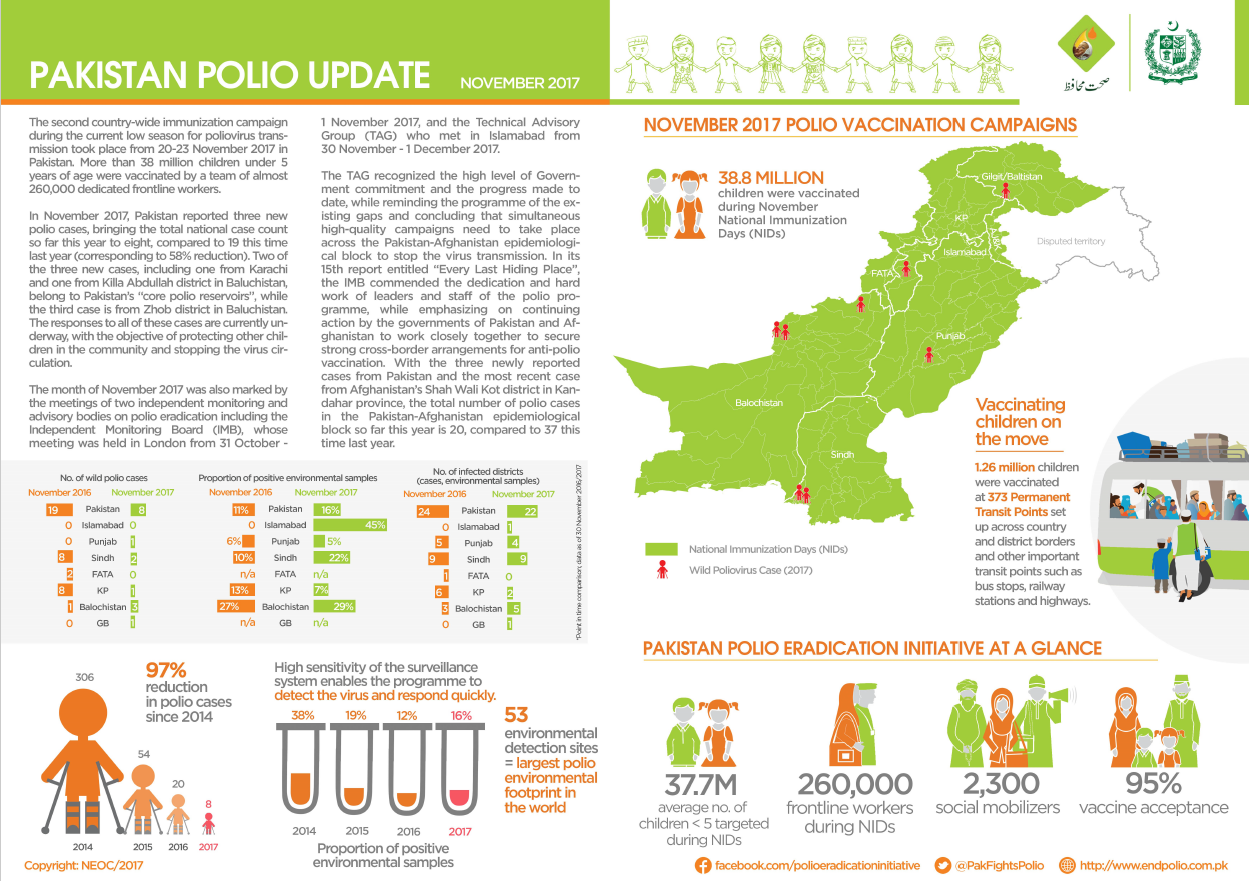
Update on polio eradication efforts in Pakistan for November 2017
Global progress and renewed commitment brought us closer than ever to a world without polio.
Member states commended for support of polio eradication efforts at the recent Islamic Conference of Health Ministers in Jeddah
€ 2 million in support pledged to help defeat last remaining reservoirs of the virus
Muslim leaders urge parents to vaccinate their children
All hands on deck to stop polio in Syria amidst conflict