Polio discussions at this year’s World Health Assembly
Meet a doctor at the frontline of polio eradication
How do vaccinators ensure that every child is reached?
In Karachi, Pakistan, Rotary PolioPlus activities are building community trust.
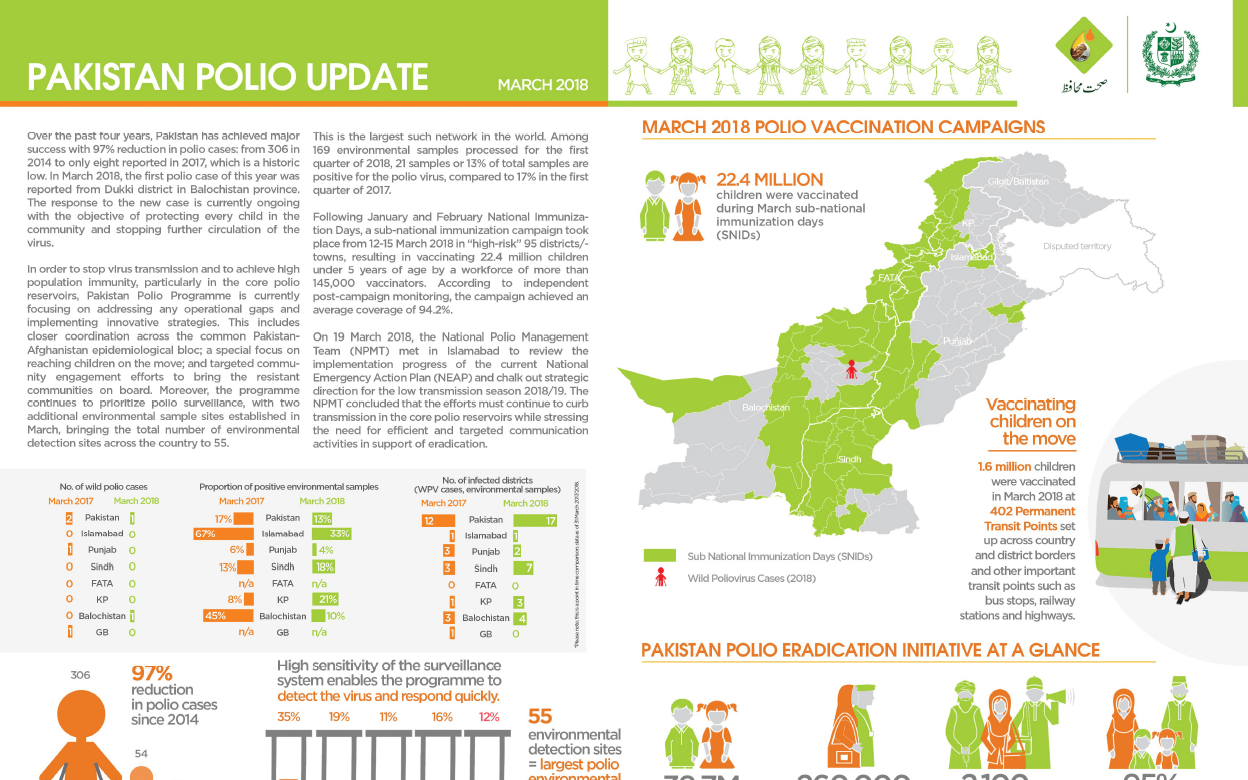
Update on polio eradication efforts in Pakistan for March 2018
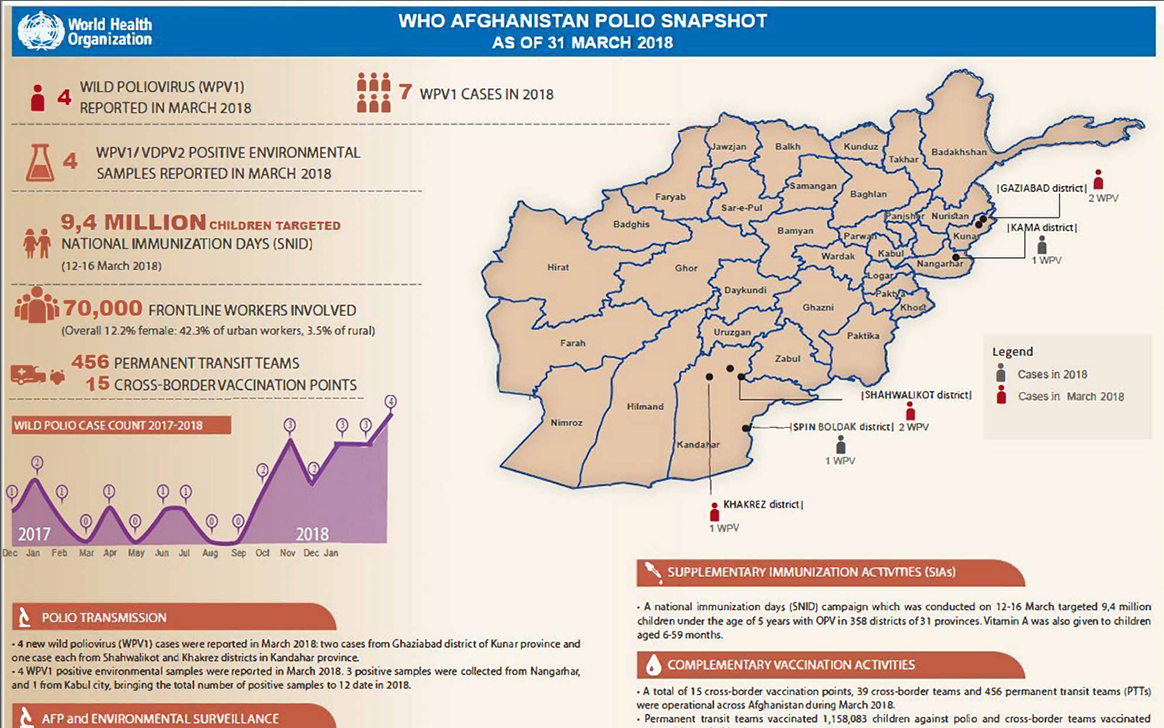
Update on polio eradication efforts in Afghanistan for March 2018
Contributions to WHO and UNICEF will help end polio in Afghanistan, and fund global eradication efforts.
Working with the polio programme opens up new opportunities for women and their communities.
A week in the life of Auta, a vaccine facilitator in Borno State
His Highness Sheikh Mohamed bin Zayed Al Nahyan, Crown Prince of Abu Dhabi, disburses final US$12 million of US$120 million commitment made...
Towards a polio-free Africa: A chat with Professor Rose Leke, Chair of the African Regional Certification Commission.
Gates and Dangote emphasized the need to eradicate polio, strengthen routine immunization, and improve primary health care.
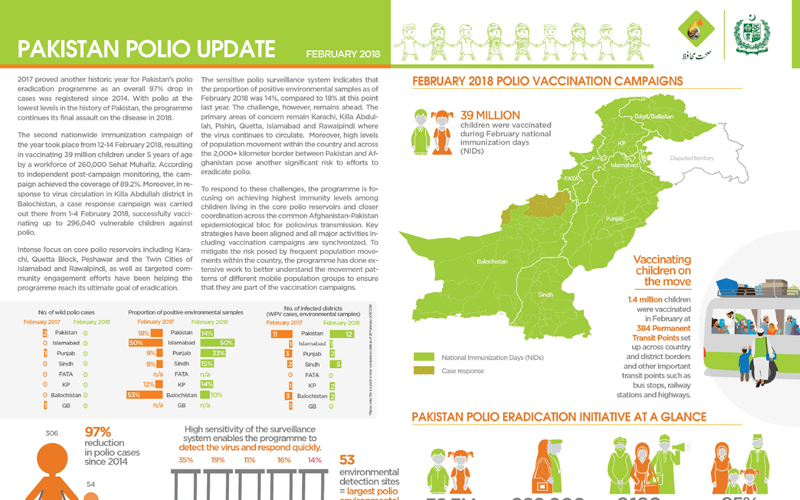
Update on polio eradication efforts in Pakistan for February 2018
In Pakistan and across the world, the poliovirus surveillance system and laboratory network are critical to eradication efforts.
What does it take to vaccinate every child in Afghanistan?
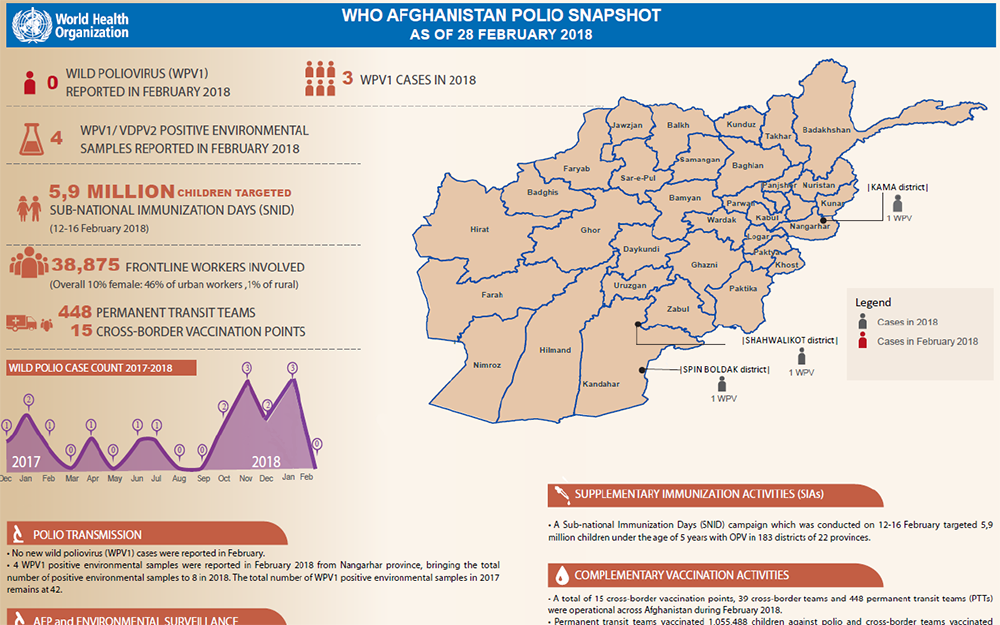
Update on polio eradication efforts in Afghanistan for February 2018
In Nigeria, experts from the frontline of polio eradication are helping to end other disease outbreaks.
In Nigeria, dedicated female mobilizers are critical in the fight against polio.
In eastern Afghanistan, one family is helping to vaccinate every last child in their community
US$ 3.2 million pledged for equipment to help detect the last remaining reservoirs of the virus.
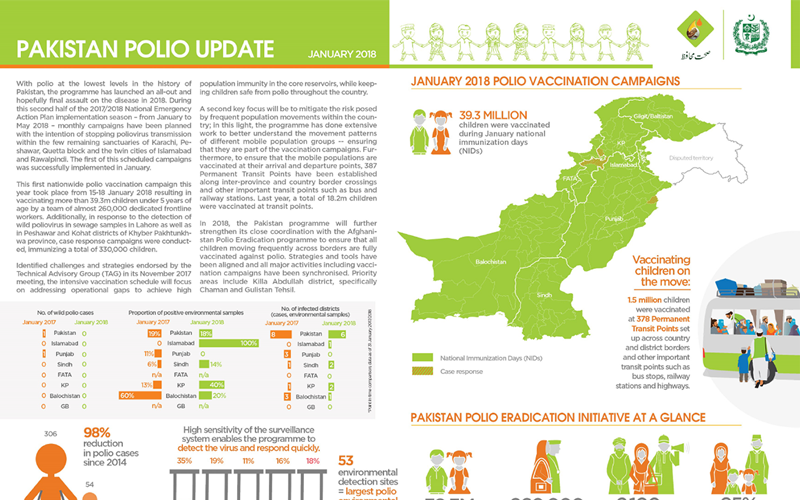
Update on polio eradication efforts in Pakistan for January 2018
The strong polio eradication infrastructure in Borno is supporting Nigeria to vaccinate over eight million people against yellow fever.
In Afghanistan, frontline health workers explain to parents why the polio vaccine must be delivered multiple times
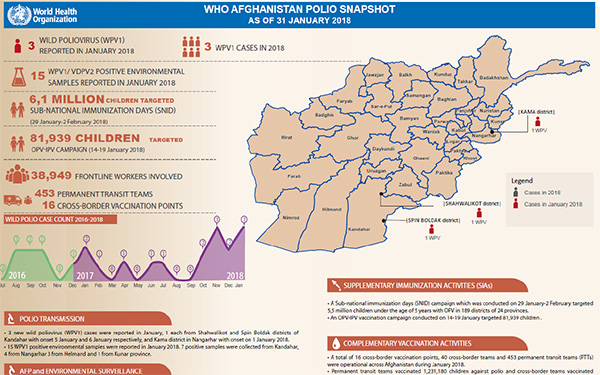
Update on polio eradication efforts in Afghanistan for January 2018
The polio surveillance system is finding the virus in the most challenging areas so that children can be protected and polio stopped for goo...