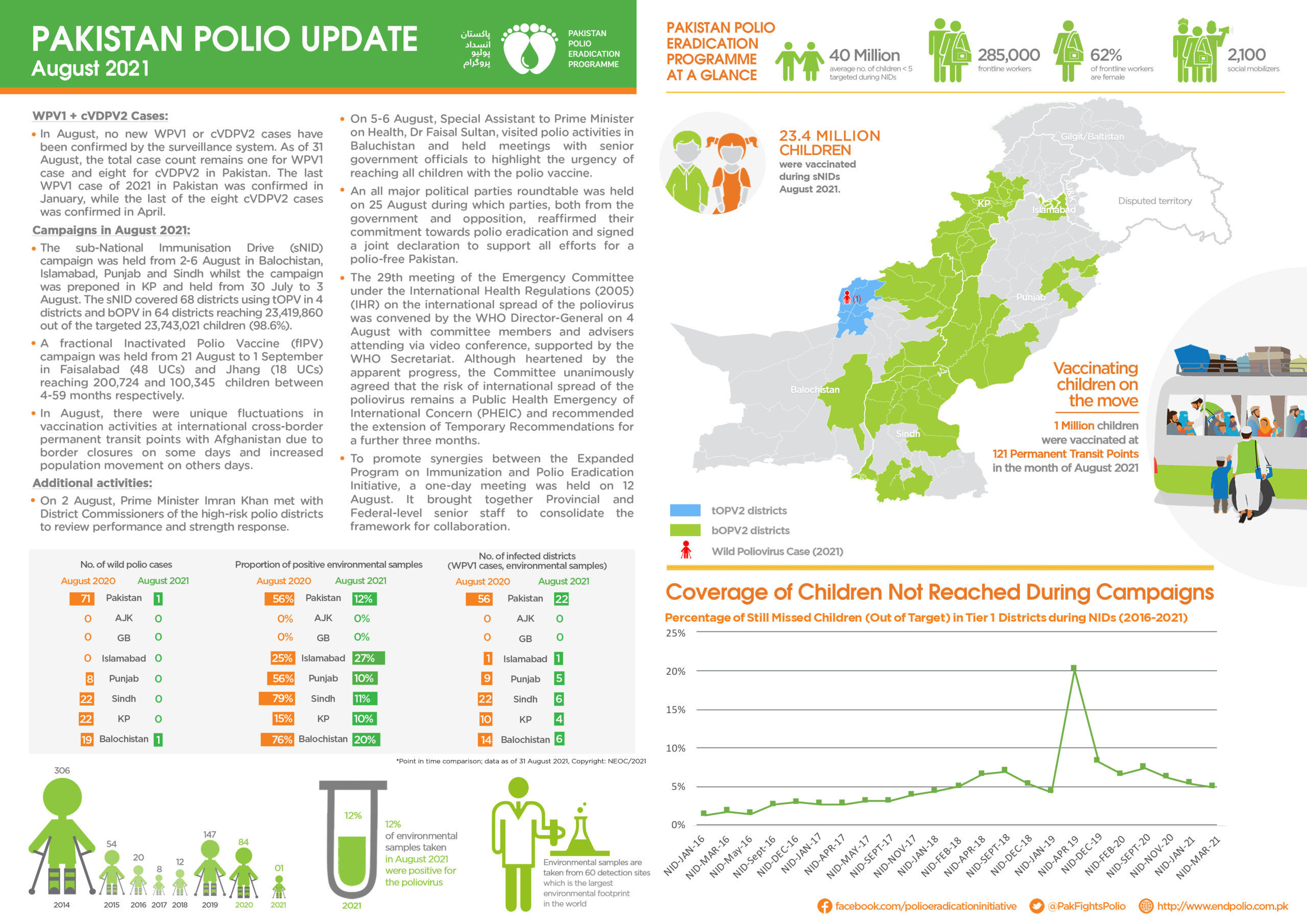
Update on polio eradication efforts in Pakistan for August 2021
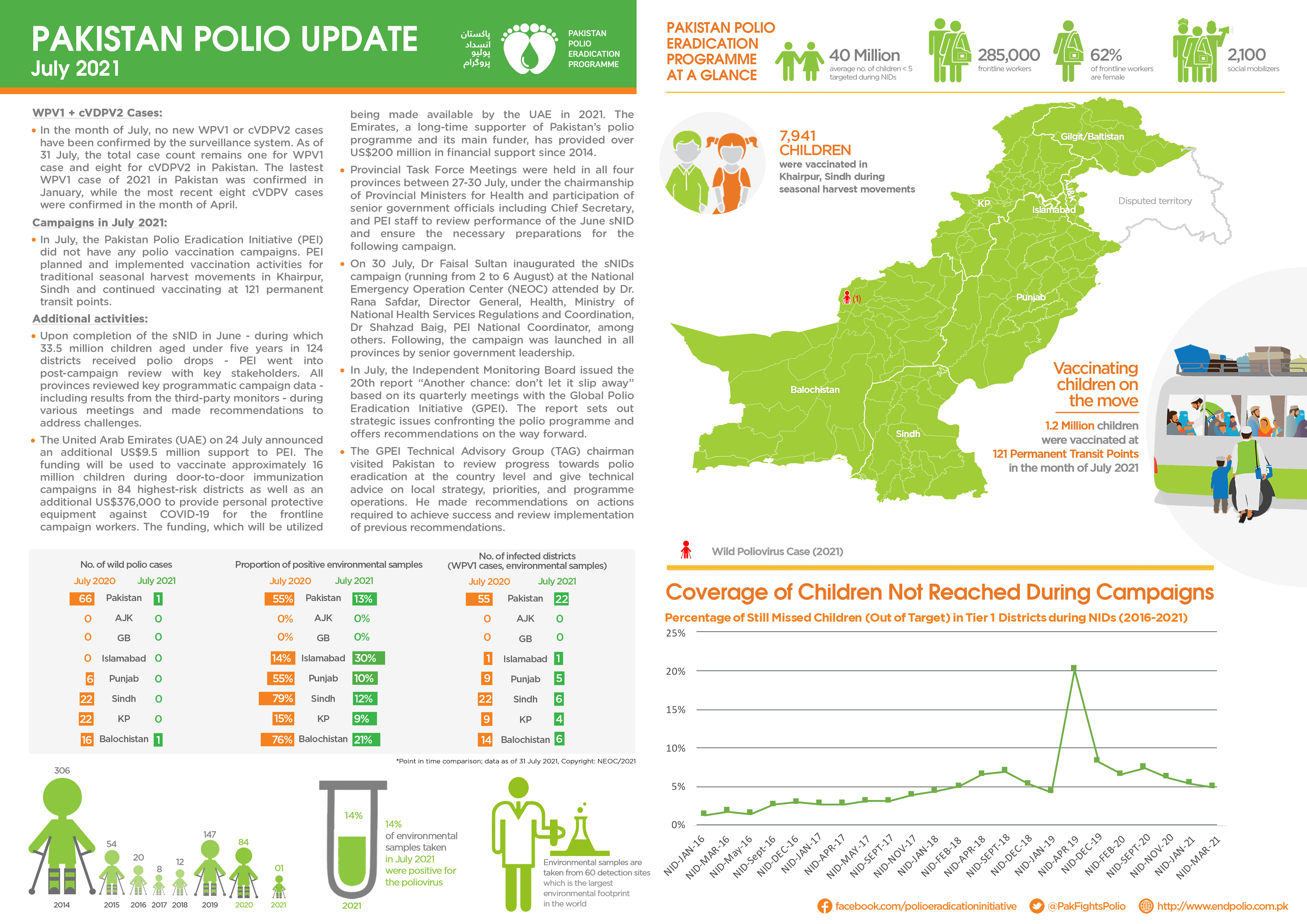
Update on polio eradication efforts in Pakistan for July 2021
Update on polio eradication efforts in Afghanistan for May 2021
Update on polio eradication efforts in Pakistan for May 2021
Update on polio eradication efforts in Afghanistan for April 2021
Somalia’s outbreak of circulating vaccine-derived poliovirus type 3 (cVDPV3) has been successfully stopped, with no international spread
Vaccinators tackle winter conditions and challenging contexts during Afghanistan’s last polio campaign of the year.
After a pause in polio campaigns due to COVID-19, Chad and other African Region countries strive to boost immunity
Community mobilizers build trust with communities ahead of crucial vaccination campaigns.
Joint efforts help reach every child with polio vaccine.
Integrated polio and measles campaign protects thousands of children.
Locally recruited health workers in Pakistan lead efforts to engage with families.
Update on polio eradication efforts in Pakistan for July 2020
Dr. Ana Elena Chevez has a message for a new generation of women public health leaders.
Vaccinators aim to fill urgent immunity gaps that have widened in the under-five population.
While the COVID-19 response dominates community health concerns, every missed opportunity for vaccination puts the fragile gains made agains...
Update on polio eradication efforts in Afghanistan for May 2020
Dr Fiona Braka, Immunization Team Lead for WHO Nigeria, speaks about fighting polio outbreaks and toppling gender barriers.
US$ 8.8 billion pledged to fund immunization through Gavi, the Vaccine Alliance.
We join Joana on a vaccination day in Happyland, one of the poorest and most densely populated areas of the city.
Update on polio eradication efforts in Afghanistan for April 2020
Update on polio eradication efforts in Pakistan for March 2020
Thanks to the leadership of His Highness Sheikh Mohamed bin Zayed Al Nahyan, Crown Prince of Abu Dhabi, millions of children in Pakistan hav...
A reminder of why vaccines are so important.
Update on polio eradication efforts in Afghanistan for March 2020