As 2022 draws to a close, independent technical bodies from key epi-centres dive deep on what it will take to achieve success in 2023
Together, we can end polio!
Tuesday 11 October 2022
The Republic of Sudan closed a polio outbreak on 15 September 2022. It had paralyzed 58 children across 42 districts before it stopped circu...
29 July 2022
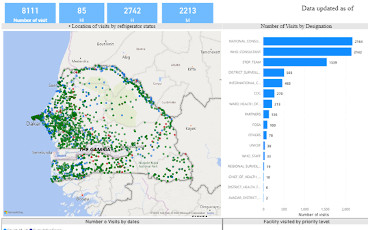
WHO Geographic Information System (GIS) equips over 200 specialists across Africa with essential digital mapping and Mobile Health skills to...
With cVDPV1 and cVDPV2 outbreaks unfolding against the backdrop of a major humanitarian crisis, polio surveillance has never been tougher –...
New guidance anticipated to quicken progress in achieving necessary safeguards
G7 and Commonwealth Heads of Government call for strengthened support to global polio eradication effort
22 June 2022
Medical doctors and religious teachers play a crucial role in building trust and convincing families to vaccinate their children against pol...
The first supplementary polio campaign in eight years puts caregivers to the test
Ananda talks about development of the nOPV2 vaccine its pathway to rollout, and field performance
18 May 2022
13 May – Ramallah
The support of community leaders and influencers is crucial in motivating parents and caregivers to vaccinate their children against polio
An outbreak response assessment led by WHO on 11 to 15 April 2022 concluded that poliovirus is no longer circulating in Tajikistan, and ther...
High-level summit held to take urgent action to end polio in country
Local health authorities conducting investigations to determine source of virus and potential risk of further spread
1 March 2022
Insecurity and displacement increase risk of diseases such as polio
Members issue two statements on Yemen and Afghanistan calling for uninterrupted access for vaccinations to all children
From a remote village in Malawi called Chinthenche to Zambia, Ethiopia, Nigeria, and finally the WHO Regional Office for Africa.
cVDPV2 outbreak response continues in the country
2021 may go down in history as the turning point in the global effort to eradicate polio.