Polio eradication staff support COVID-19 response
Exploring the ‘plus’ in PolioPlus.
Ten years, ten heroes of polio eradication. We revisit the stories of incredible people all over the world dedicated to ending polio.
Part three in our series on the ‘plus’ in PolioPlus.
WHO invites filmmakers to participate in our inaugural film festival
Part two in our series on the ‘plus’ in PolioPlus.
In the run up to the GPEI Pledging Event in November, the G20 Okayama Declaration emphasizes ending polio and delivering vaccines to all.
A series on the ‘plus’ in PolioPlus: preventing other diseases
Form by form, campaign by campaign, data handlers like Jan, Ali, and Bilal are helping to end polio.
UAE, partners, and donors in attendance as Global Polio Eradication Initiative introduces 2019-2023 Investment Case
Grassroots efforts got Nigeria over the barriers to polio vaccination
Political will apparent for Universal Health Coverage, Primary Health Care and polio eradication with Japan’s leadership
Decades-long polio infrastructure has spill-over benefits across larger public health interventions
Resilience and resolve are the keywords for women eradicating polio
On International Women’s Day, we celebrate the role of women in the polio eradication efforts in Pakistan
A look at some of the women in Somalia’s polio programme
Progress in the challenging last mile of eradication
Over 140 public health experts from 22 countries gather at the 6th Regional Meeting on Polio in Guatemala
New collection of 30+ multimedia stories from Afghanistan, Pakistan and India now available on GPEI website
Over 31 million children will be vaccinated against measles in Pakistan in a countrywide immunization campaign supported by the polio progra...
Group continues its historical support
Anand Balachandran, former Coordinator Polio Transition, speaks to us about ensuring the infrastructure built up to eradicate polio will con...
Afia is part of one of the biggest female work forces in Afghanistan.
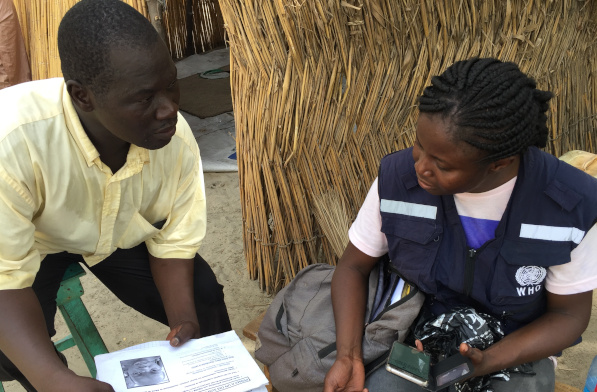
Across the Lake Chad Basin, e-Surve technology is revolutionizing the way that the polio programme conducts disease surveillance
Honorine Mollard Billard, Polio Eradication Officer at WHO, speaks to us about critical country support to vaccination campaigns in Lao PDR...