The preventive vaccination campaign led by Pakistan in partnership with the World Health Organization protected 34 million children against...
More often than not, the road to a meaningful triumph is a bumpy one.
Momentous global effort enables record-breaking milestone for polio and immunisation
Polio programme assessed by experts at the global immunization meeting
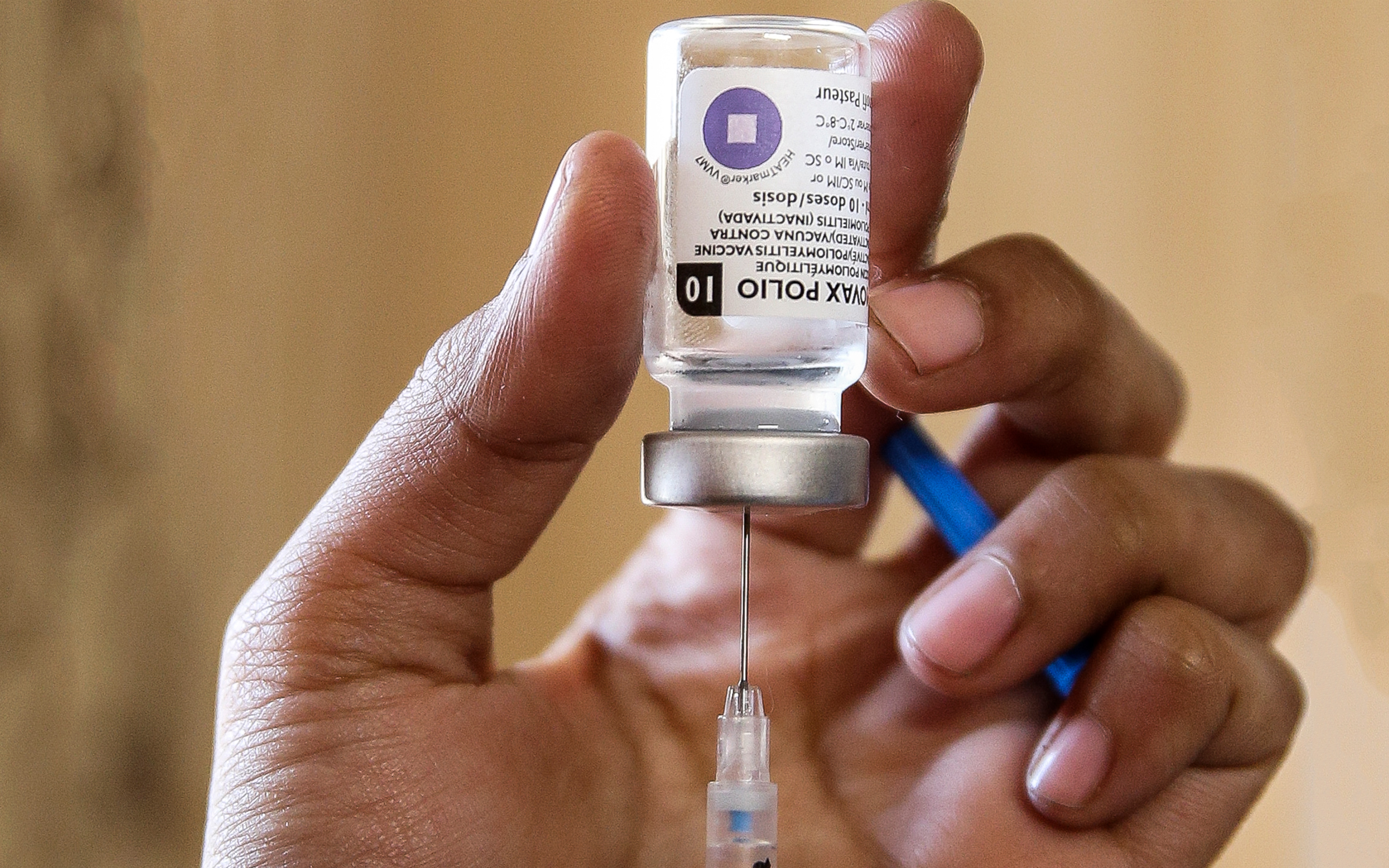
New study shows fractional dose IPV (fIPV) boosts mucosal immunity in previously OPV-vaccinated children.
Flexible support to Nigeria also approved.
Sweden is the first country to formally engage in the global poliovirus containment process
Why we are developing new polio vaccines for the post-eradication era.
Polio can’t be cured, but it can be prevented. Two important tools help to prevent polio – two safe, effective vaccines. Find out about the...
Carolyn Sein, Technical Officer for the GPEI programme, talks to us about circulating vaccine-derived polioviruses, and the important differ...
Ministries of health from around the world call for urgent measures to secure lasting polio-free world