Last year, the Polio Oversight Board visited Pakistan twice, acknowledging the unprecedented support and commitment by all stakeholders to e...
From the field: polio vaccination campaign in Pakistan
Pakistan’s polio program has launched a novel initiative to reach children of nomadic families with polio and essential vaccines so that the...
How the polio program came together to help flood-affected frontline workers
21 March 2023
On Tuesday 28 February 2023, ministers and high-level delegates from across the Eastern Mediterranean Region participated in the seventh mee...
At the workshops, women health workers were the chief guests while everyone else had one job: to listen.
Seventh meeting of the Regional Subcommittee for Polio Eradication and Outbreaks - 28 February 2023
There’s commitment at every level to eradicate polio.
At WHO Executive Board, experts discuss concrete ways to tackle last remaining polio strong-holds
16 January 2023
This snapshot shows all polio events and outbreaks that occurred/were ongoing in the Eastern Mediterranean Region (EMR) in 2022
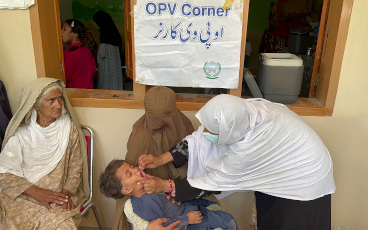
When a mother brought her young son to a clinic in Paghman, a town not far from the Afghan capital Kabul, Spogmai, a nurse on duty at the ti...
Recommendations from the international review of Afghanistan’s poliovirus surveillance system are yielding important results for the country...
As 2022 draws to a close, independent technical bodies from key epi-centres dive deep on what it will take to achieve success in 2023
ISLAMABAD, DEC 2, 2022
Together, we can end polio!
We are close to making polio the second human disease to be eradicated, but what will it take to finally consign this killer disease to the...
More than 3000 scientists and health experts from 115 countries urge the world to fully fund eradication strategy following resurgence of di...
Tuesday 11 October 2022
“Rarely have I seen such commitment and dedication as I have seen in Pakistan.”
11 October 2022
Pakistan is one of just two countries where the polio virus remains endemic. Challenges remain in identifying and vaccinating all children,...
Dr Abdinoor Mohamed, an epidemiologist tells us about his team's travel to Afghanistan to review the country’s polio surveillance system, vi...
A story of determination, friendship and support