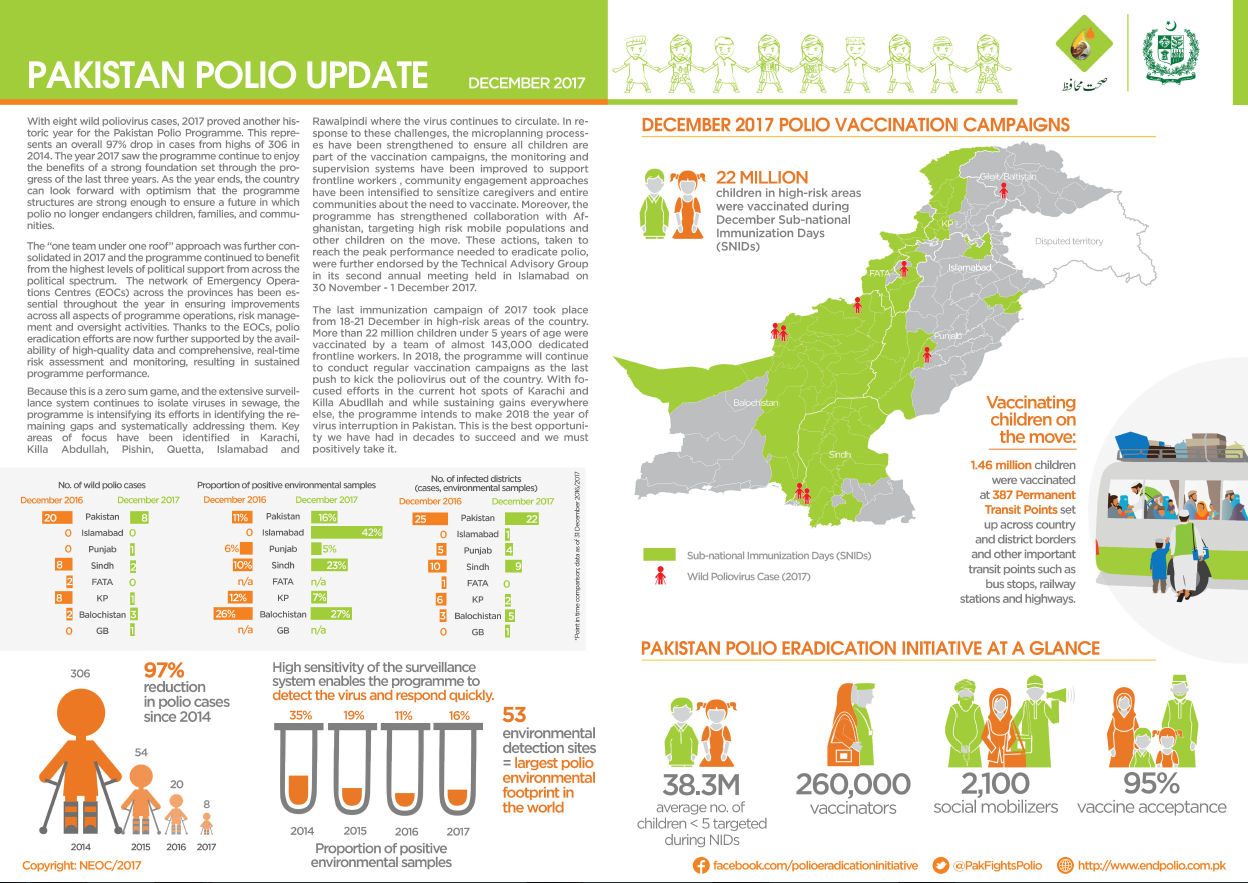
Update on polio eradication efforts in Pakistan for December 2017
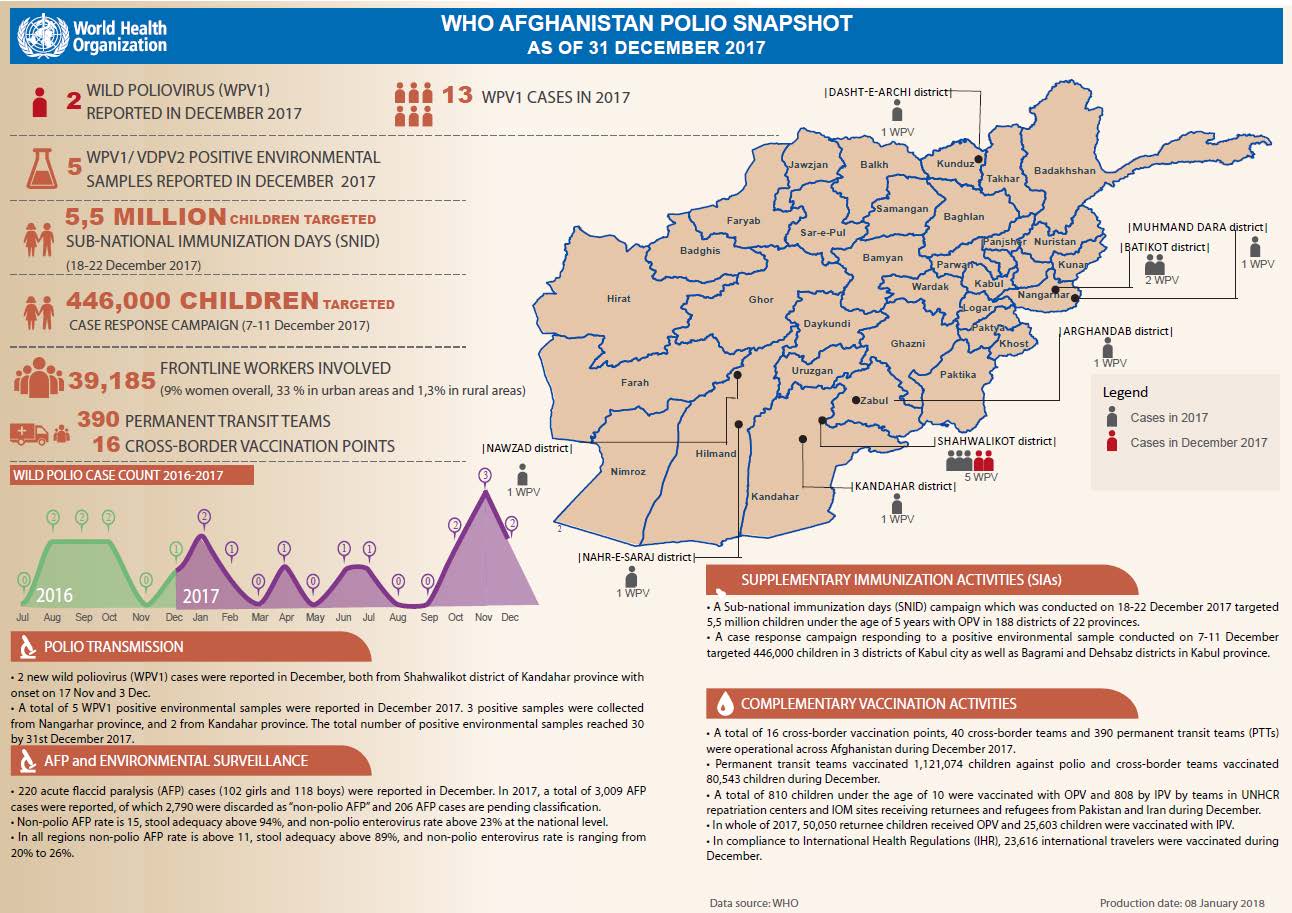
Update on polio eradication efforts in Afghanistan for December 2017
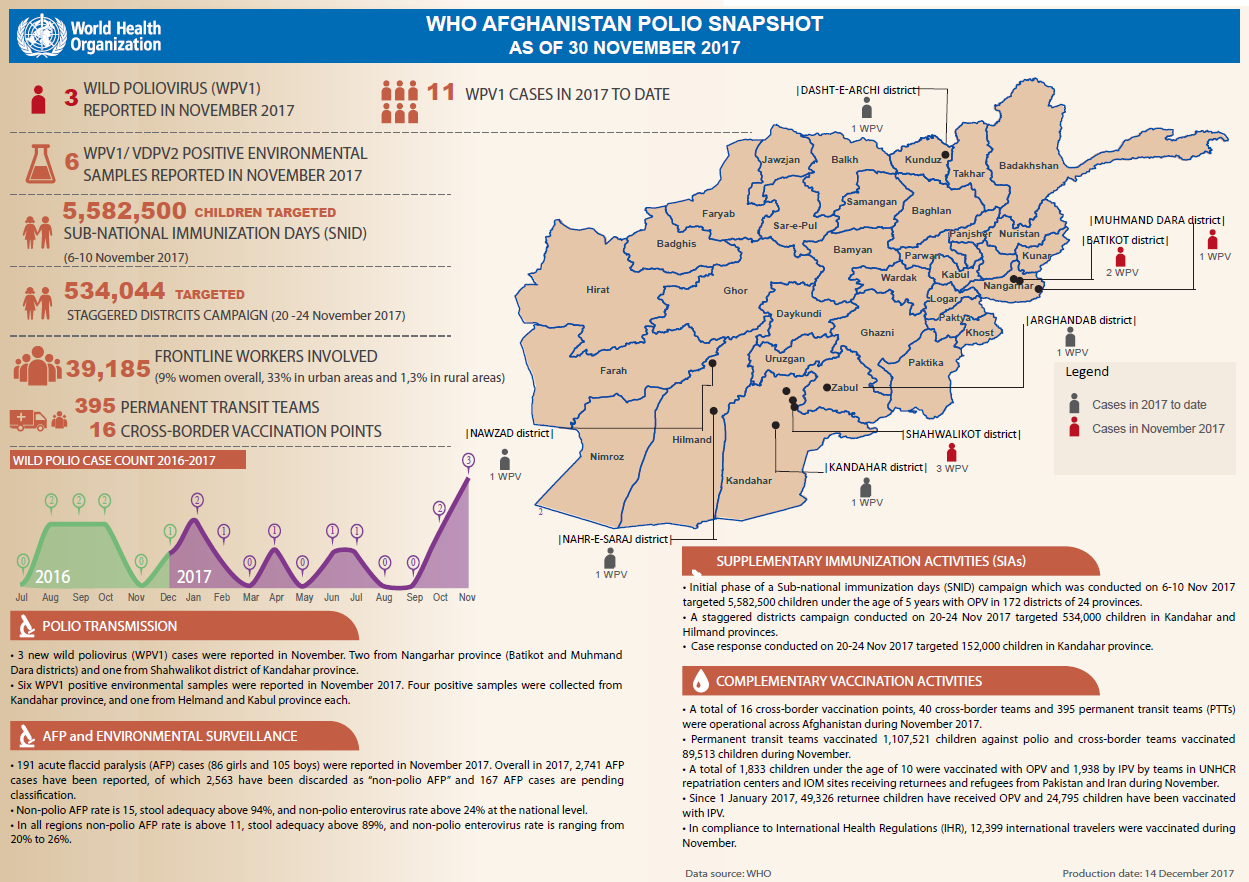
Update on polio eradication efforts in Afghanistan for November 2017
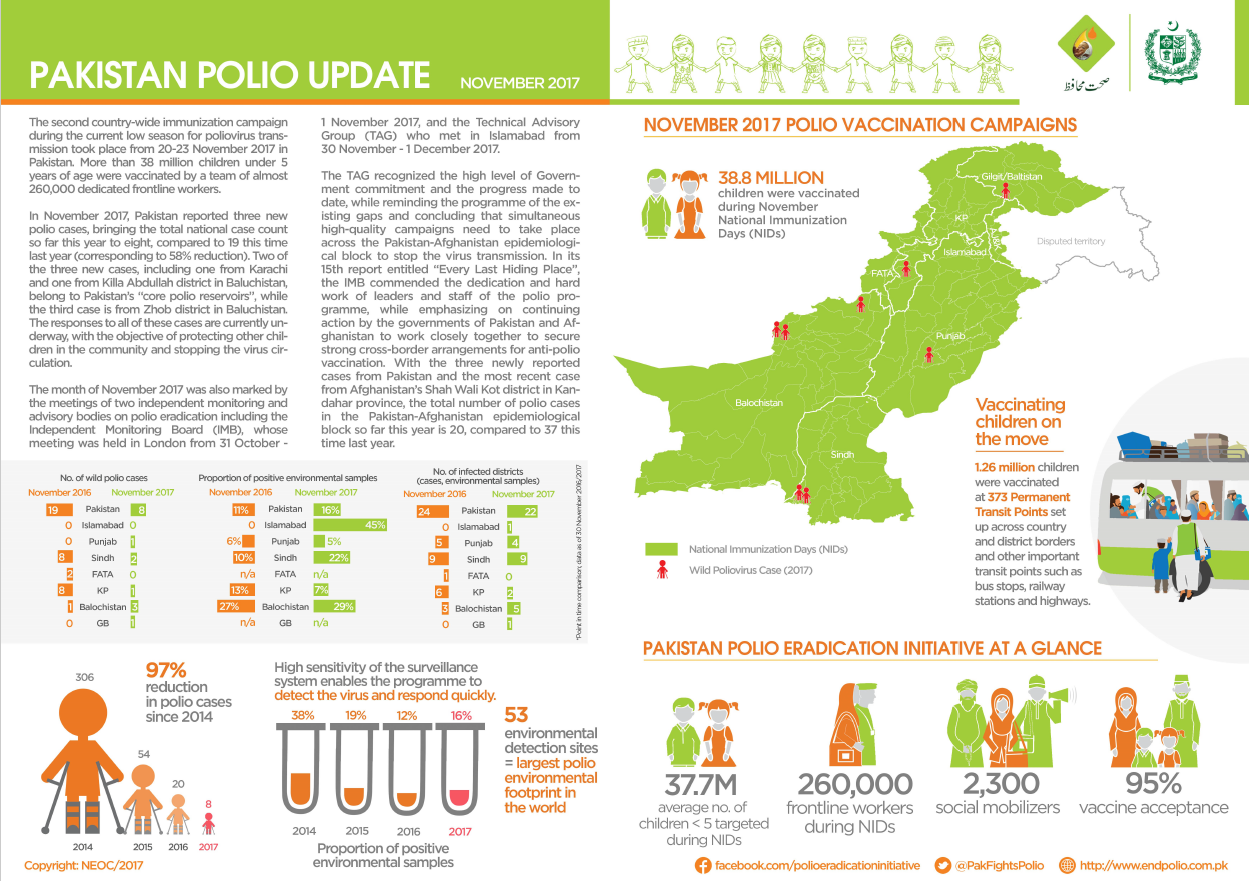
Update on polio eradication efforts in Pakistan for November 2017
Global progress and renewed commitment brought us closer than ever to a world without polio.
Member states commended for support of polio eradication efforts at the recent Islamic Conference of Health Ministers in Jeddah
€ 2 million in support pledged to help defeat last remaining reservoirs of the virus
In Pakistan, the polio eradication programme and the routine immunization programme are working hand in hand to increase vaccination coverag...
Recommendations for further interventions in Pakistan and Afghanistan as progress towards polio eradication is put under the microscope.
Muslim leaders urge parents to vaccinate their children
Giving hope for better lives to people with polio
Different methods of community engagement help to protect every child with vaccines.
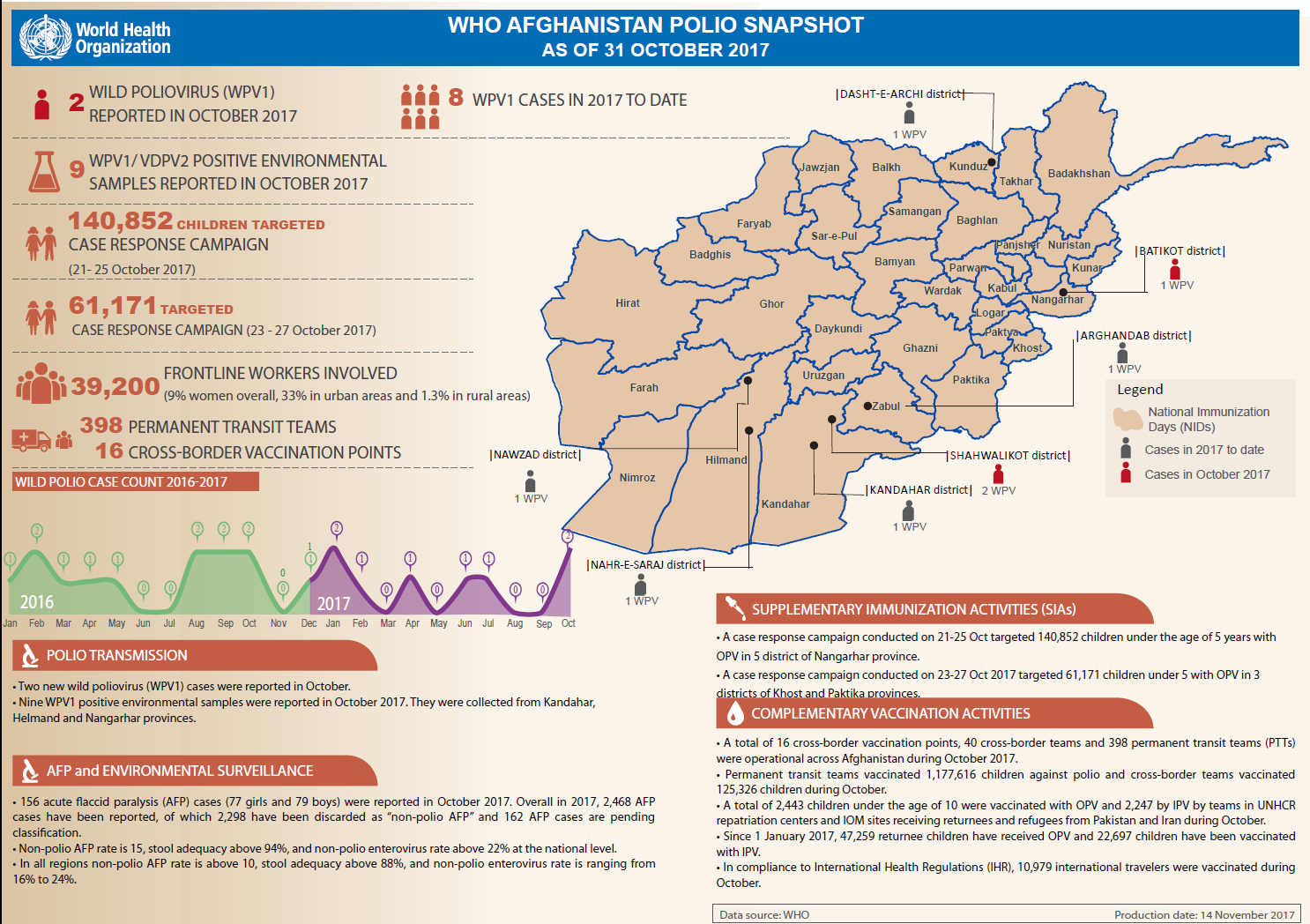
Update on polio eradication efforts in Afghanistan for October 2017
In Afghanistan, blood tests are identifying where vaccination campaigns are working, and where gaps remain to be filled.
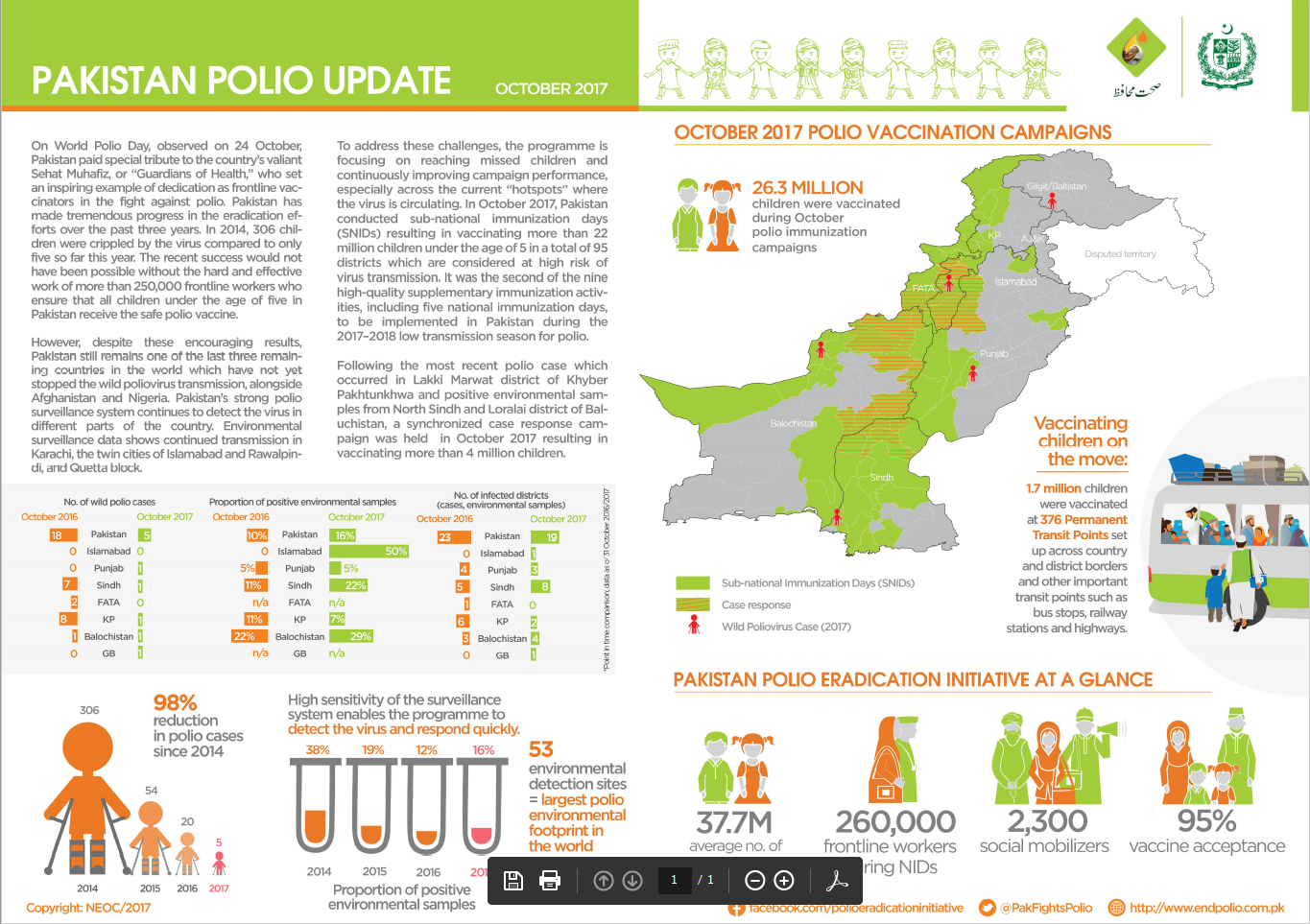
Update on polio eradication efforts in Pakistan for October 2017
On World Children’s Day we look at how the polio eradication programme contributes to ensuring children receive vital vaccines against polio...
With families on the move posing one of the biggest challenges to eradication in Pakistan, an innovative campaign is vaccinating children on...
Community health workers responding to humanitarian crisis in Nigeria are helping to stop polio and malaria hand in hand.
Abdullah Khalid is one of the hardworking vaccinators making sure that even children on the move are protected against polio.
Michel Zaffran, Director of Polio Eradication at the World Health Organization, spoke to Gavi about the difficulties in vaccinating every ch...
Polio eradicators in cities worldwide are overcoming unique challenges to stop the virus and reach every child with vaccines.
A youth circus group is encouraging vaccination and providing education in an innovative and engaging way
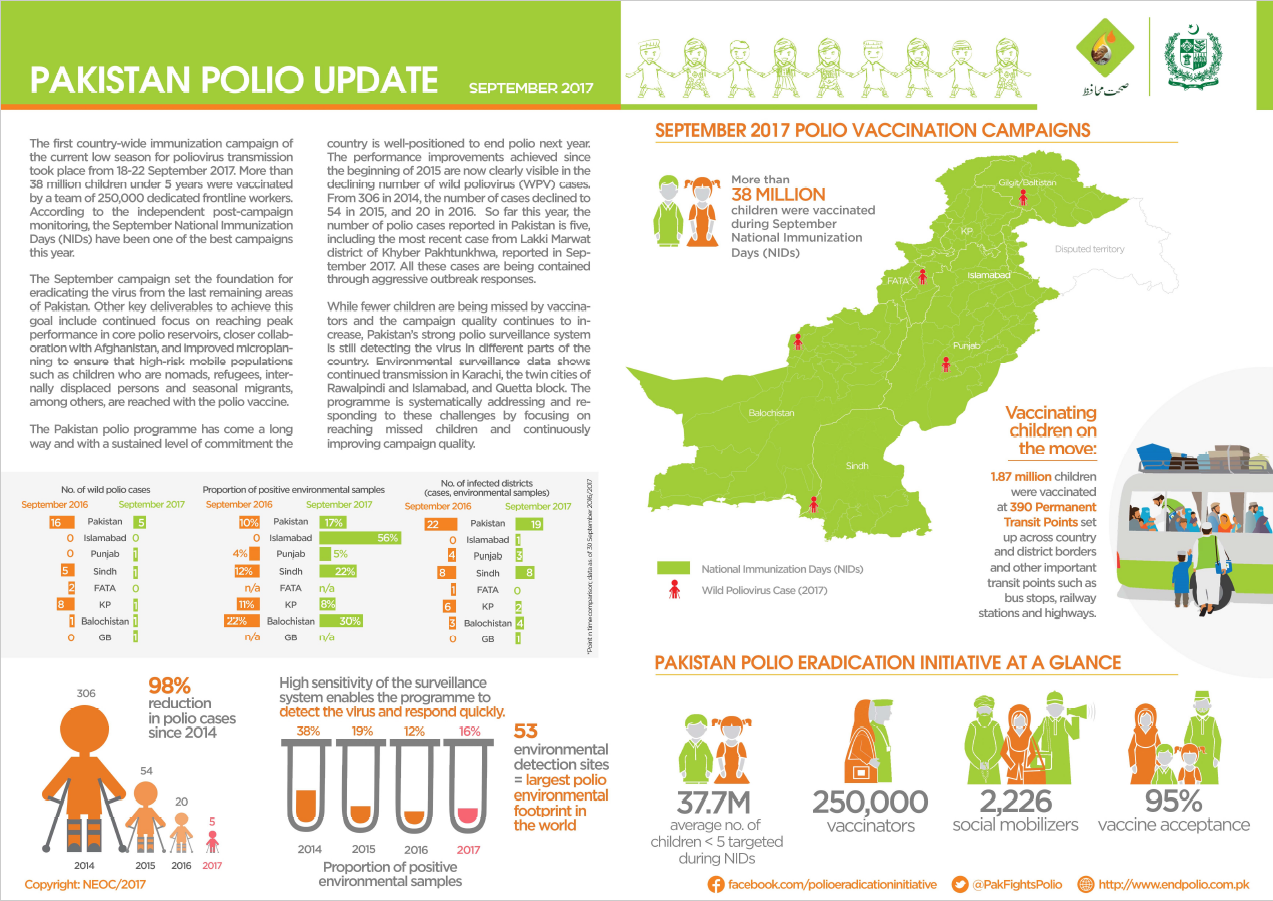
Update on polio eradication efforts in Pakistan for September 2017
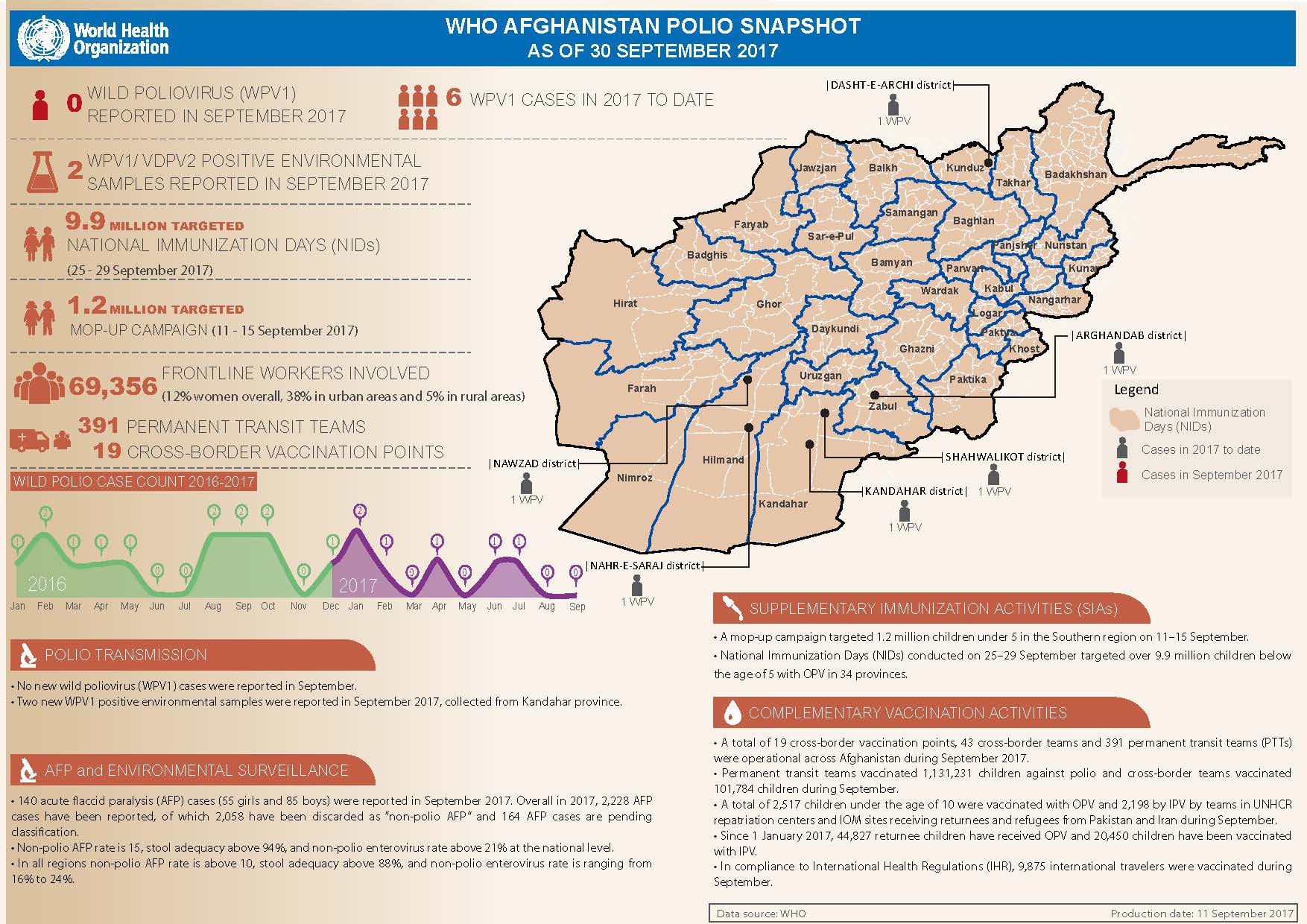
Update on polio eradication efforts in Afghanistan for September 2017