Muslim leaders urge parents to vaccinate their children
All hands on deck to stop polio in Syria amidst conflict
Different methods of community engagement help to protect every child with vaccines.
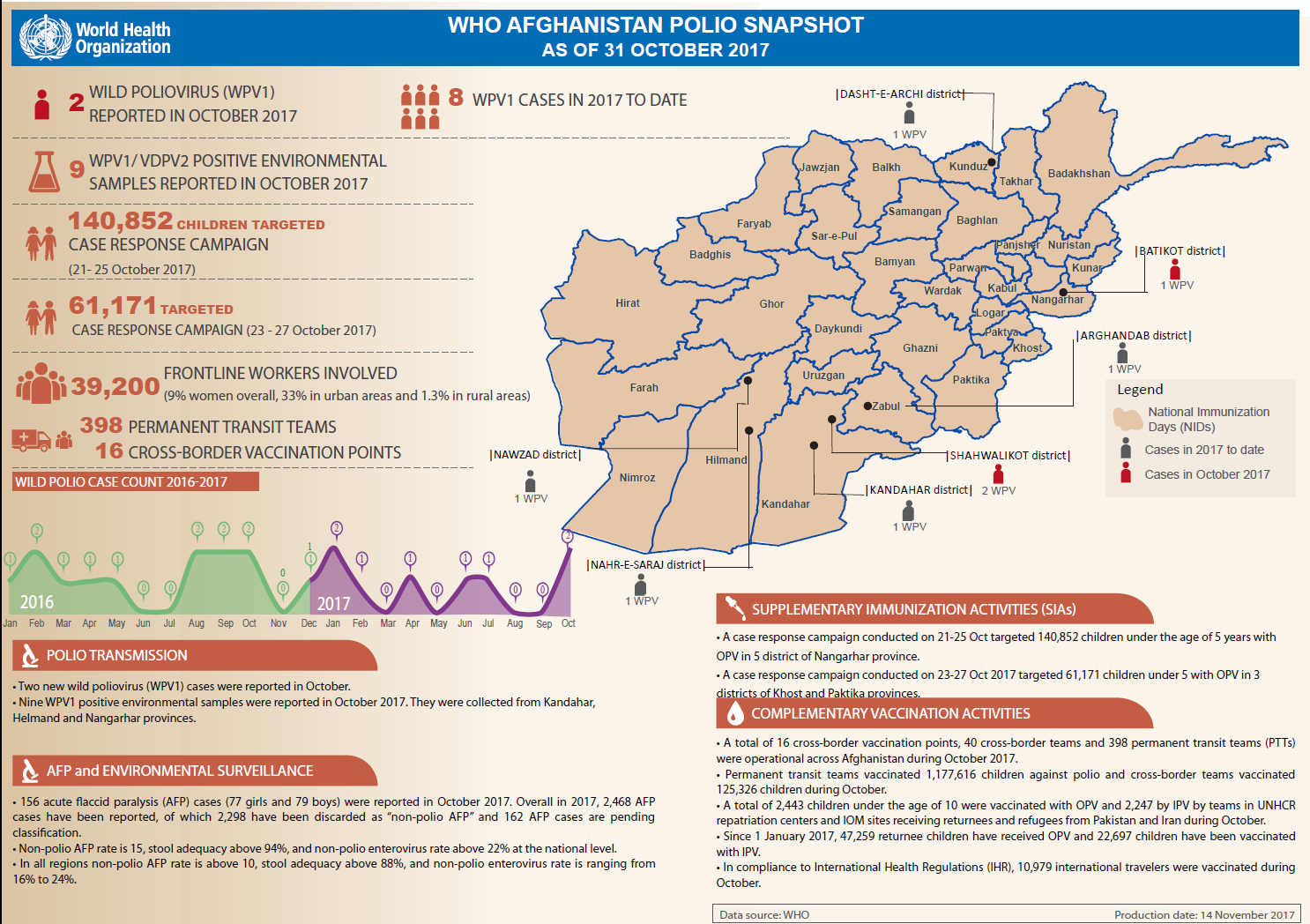
Update on polio eradication efforts in Afghanistan for October 2017
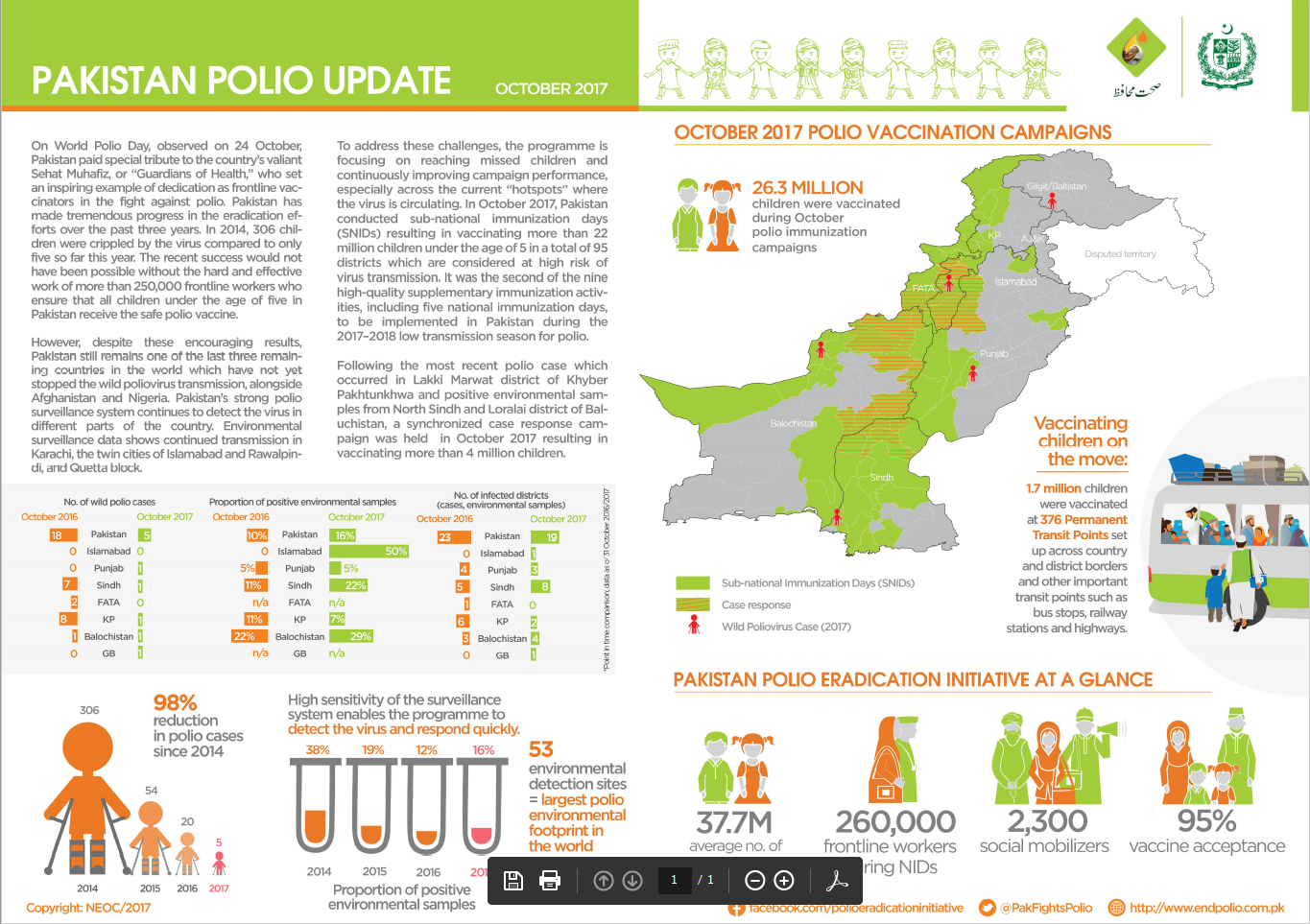
Update on polio eradication efforts in Pakistan for October 2017
On World Children’s Day we look at how the polio eradication programme contributes to ensuring children receive vital vaccines against polio...
With families on the move posing one of the biggest challenges to eradication in Pakistan, an innovative campaign is vaccinating children on...
Community health workers responding to humanitarian crisis in Nigeria are helping to stop polio and malaria hand in hand.
Abdullah Khalid is one of the hardworking vaccinators making sure that even children on the move are protected against polio.
One of an animated series on the global drive to eradicate polio.
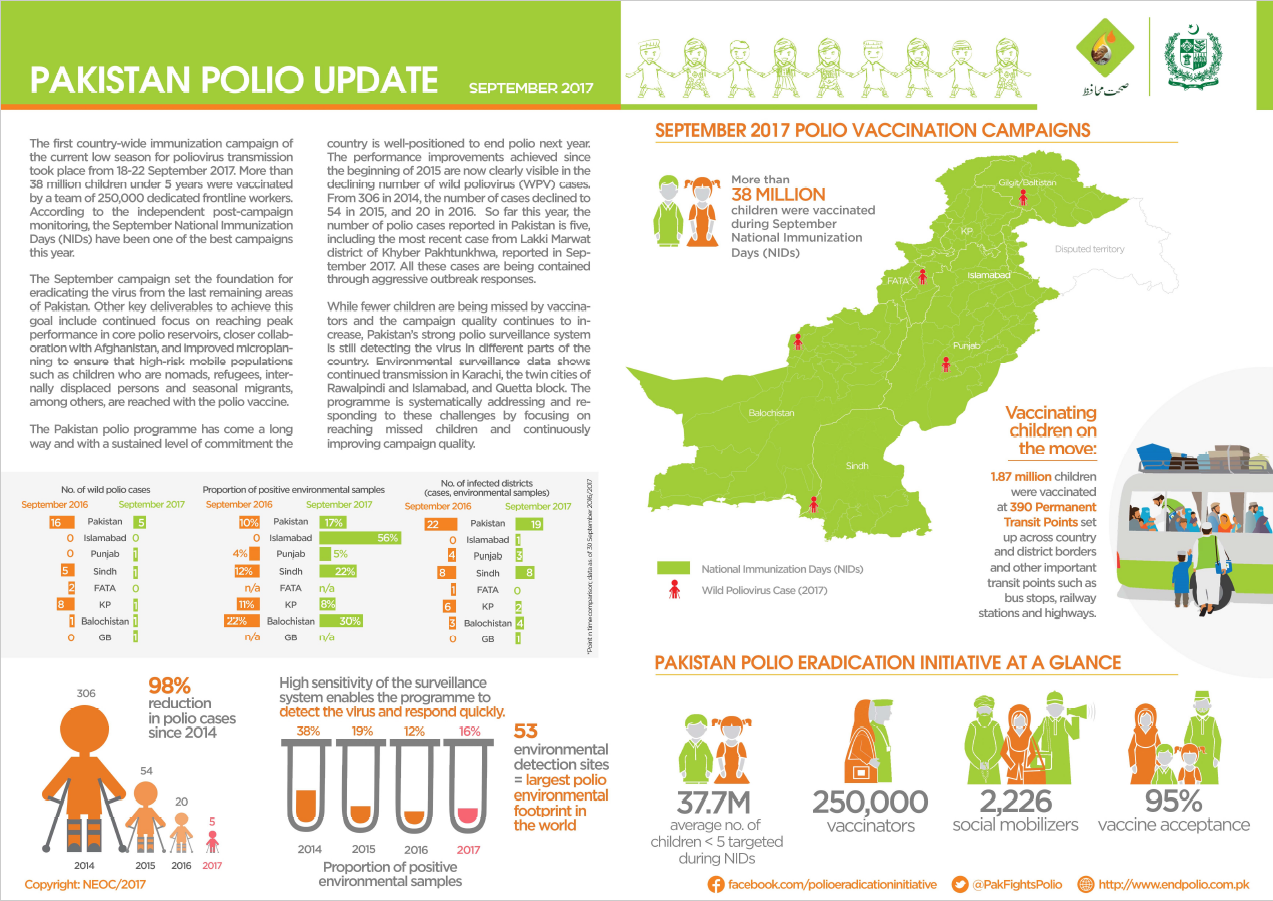
Update on polio eradication efforts in Pakistan for September 2017
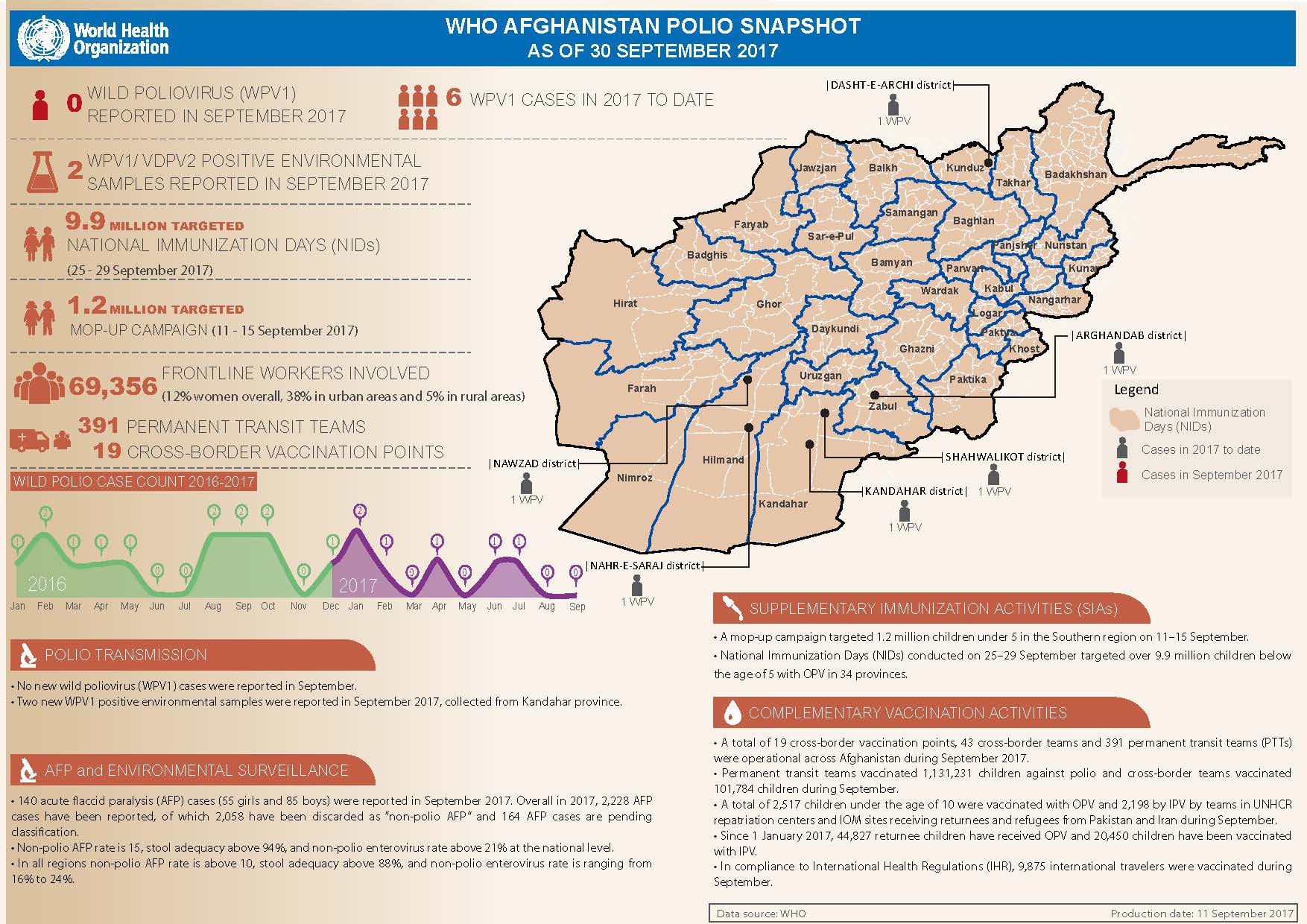
Update on polio eradication efforts in Afghanistan for September 2017
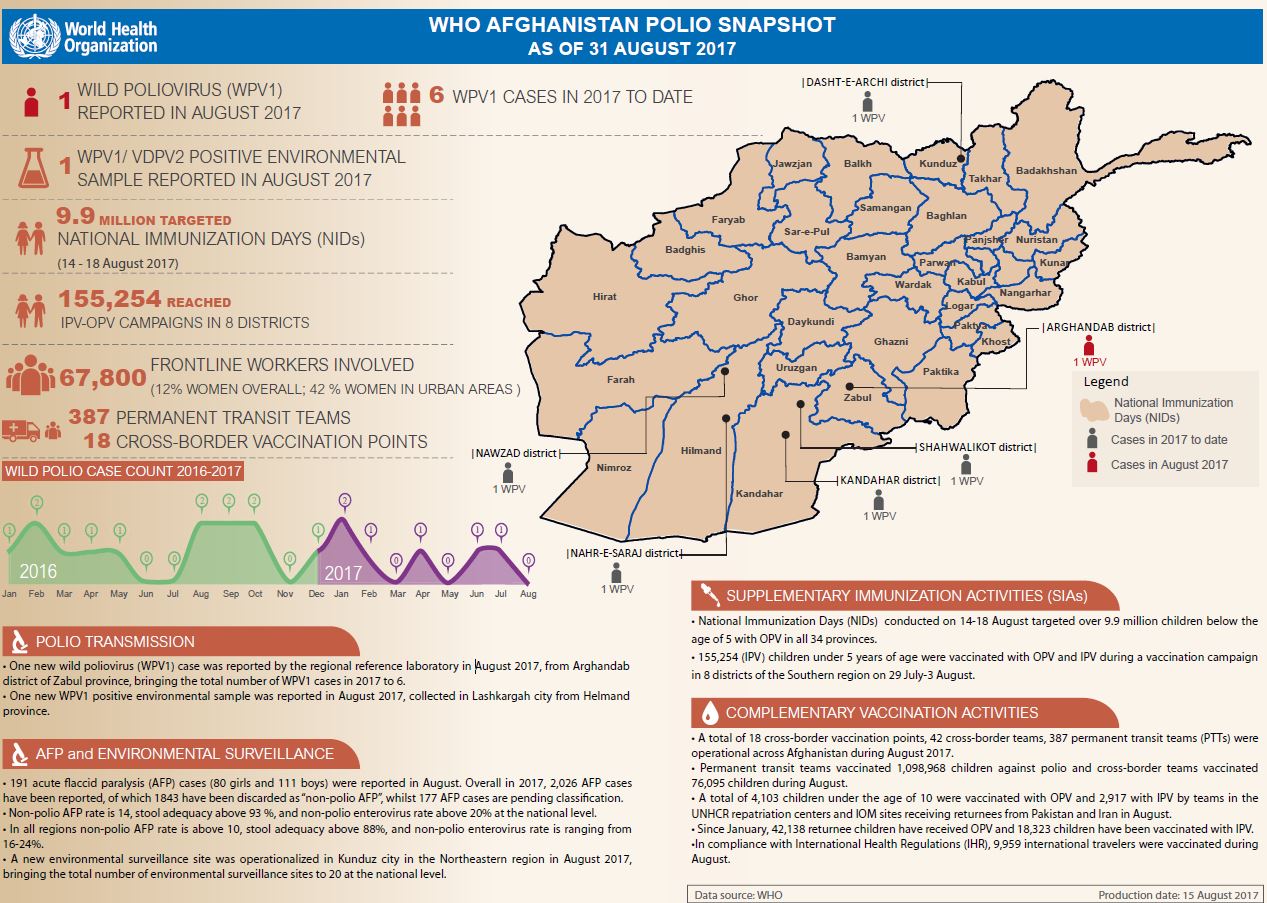
Update on polio eradication efforts in Afghanistan for August 2017
Despite challenges, polio vaccination campaigns have been carried out in Syria in response to an outbreak of vaccine-derived poliovirus
In July and August, health workers and volunteers vaccinated hundreds of thousands of children in targeted campaigns in Syria to protect the...
Polio has not been detected for a year, but that doesn't mean it’s gone
On his motorbike, Mullah Rashid criss-crosses Kandahar, talking to communities about the importance of vaccination
Adding creativity and colour to polio eradication efforts in Afghanistan.
Mountains, floods, deserts, long distances can all make it harder to reach every last child with vaccine
Before a vaccination campaign begins, health workers must piece together a huge amount of information so every last child is reached with th...
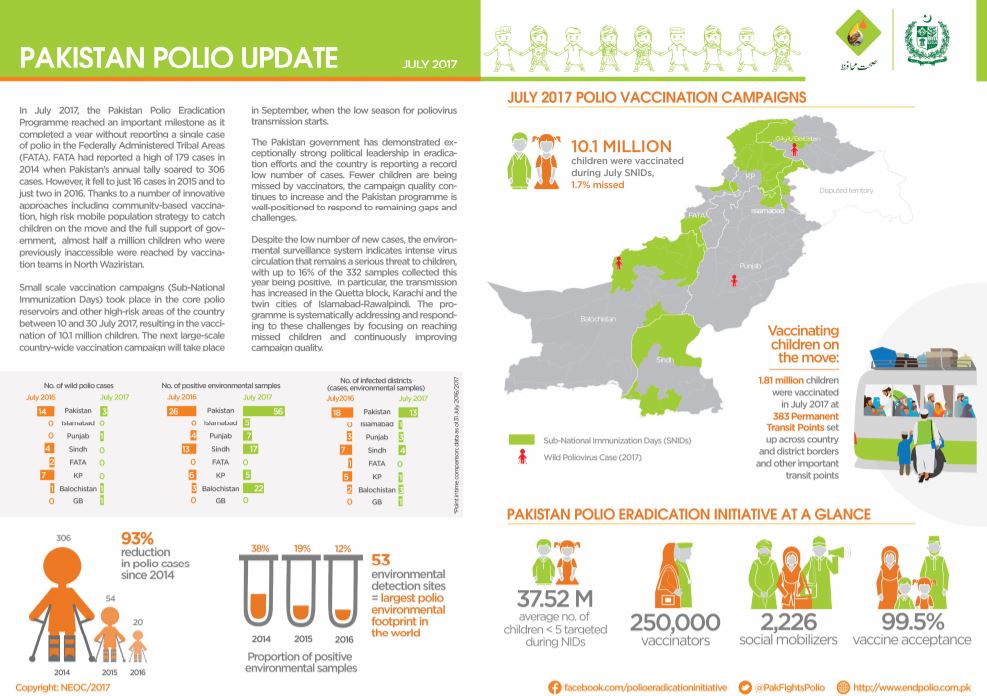
Snapshot of polio eradication efforts in Pakistan for July 2017
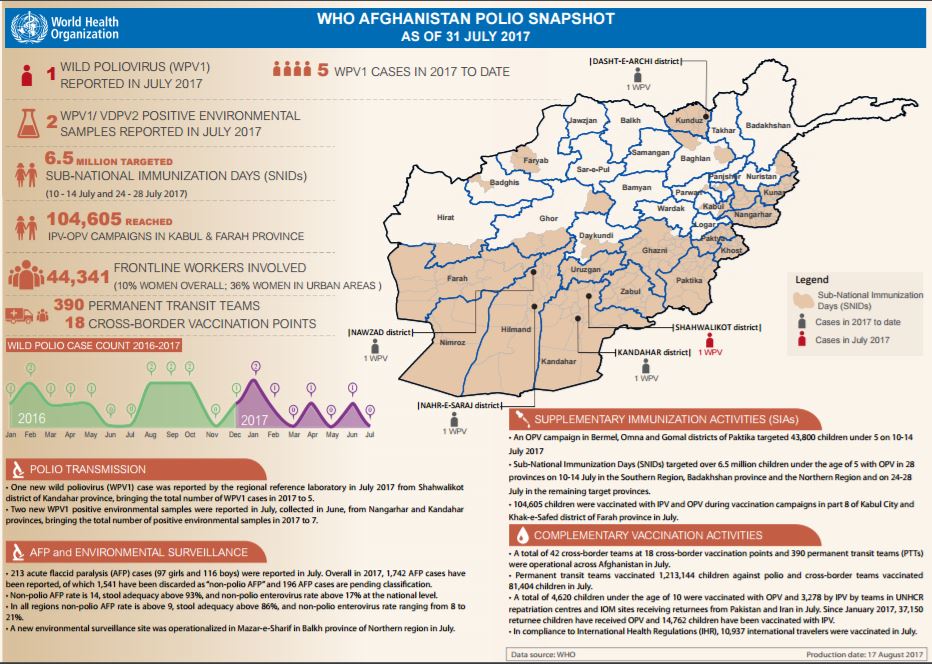
Update on polio eradication efforts in Afghanistan for July 2017
Karachi’s Khalida - forging a path to trust in vaccines