The innovations making a difference to outbreak response.
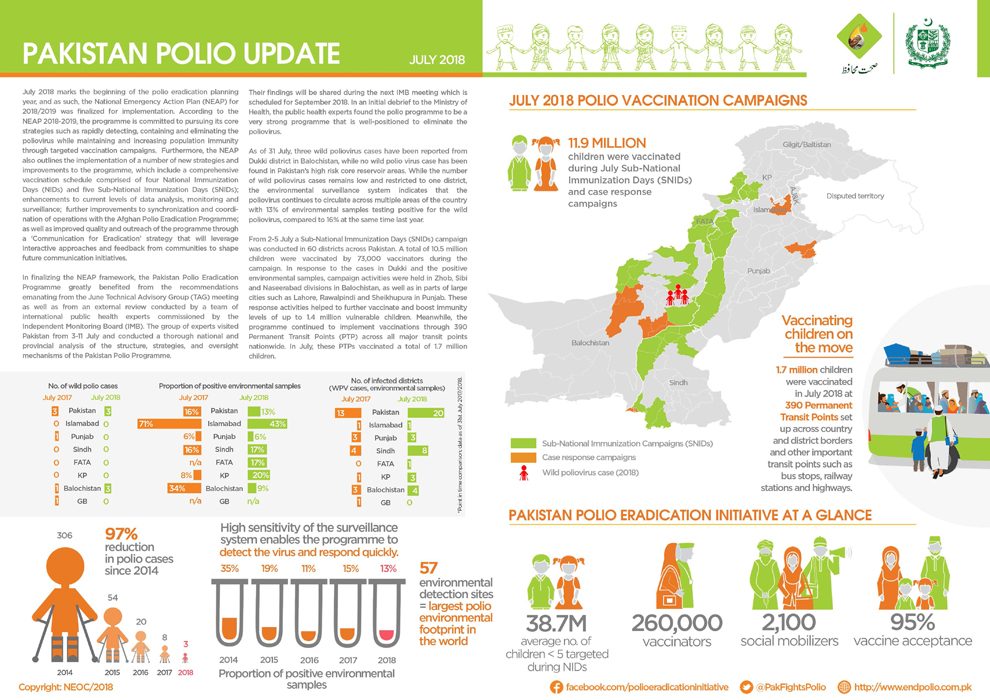
Update on polio eradication efforts in Pakistan for July 2018
Take a look at how the Papua New Guinea Government, the World Health Organization, and partners of the Global Polio Eradication Initiative a...
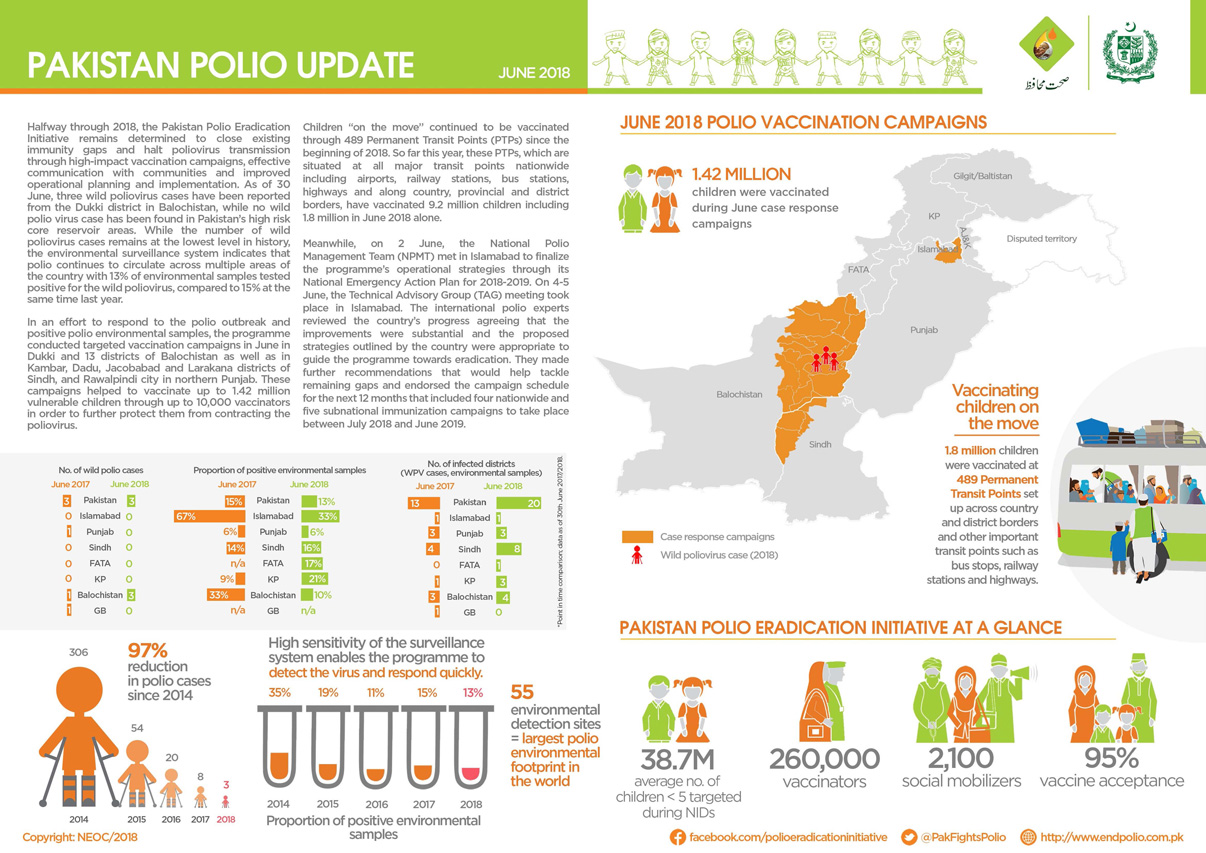
Update on polio eradication efforts in Pakistan for June 2018
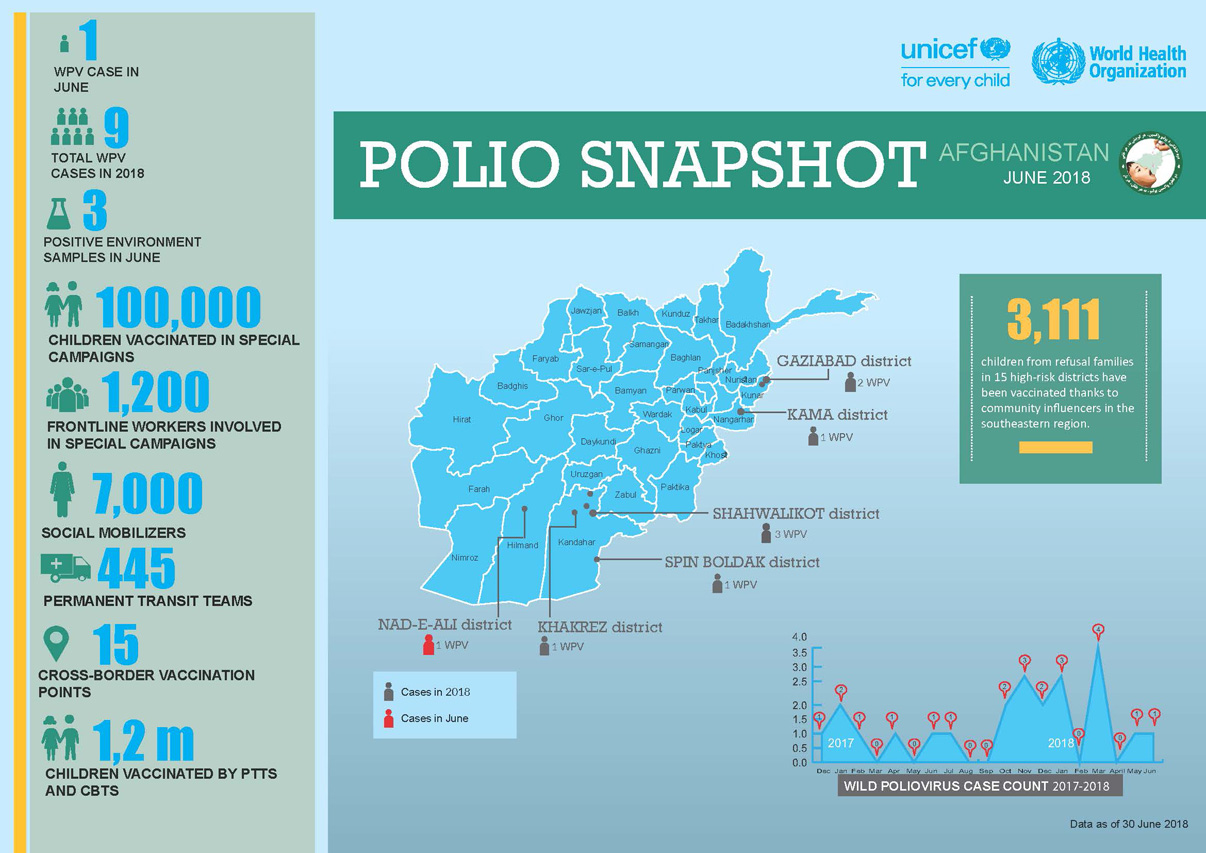
Update on polio eradication efforts in Afghanistan for June 2018
Afia is part of one of the biggest female work forces in Afghanistan.
How a vaccine refuser became an advocate for polio eradication.
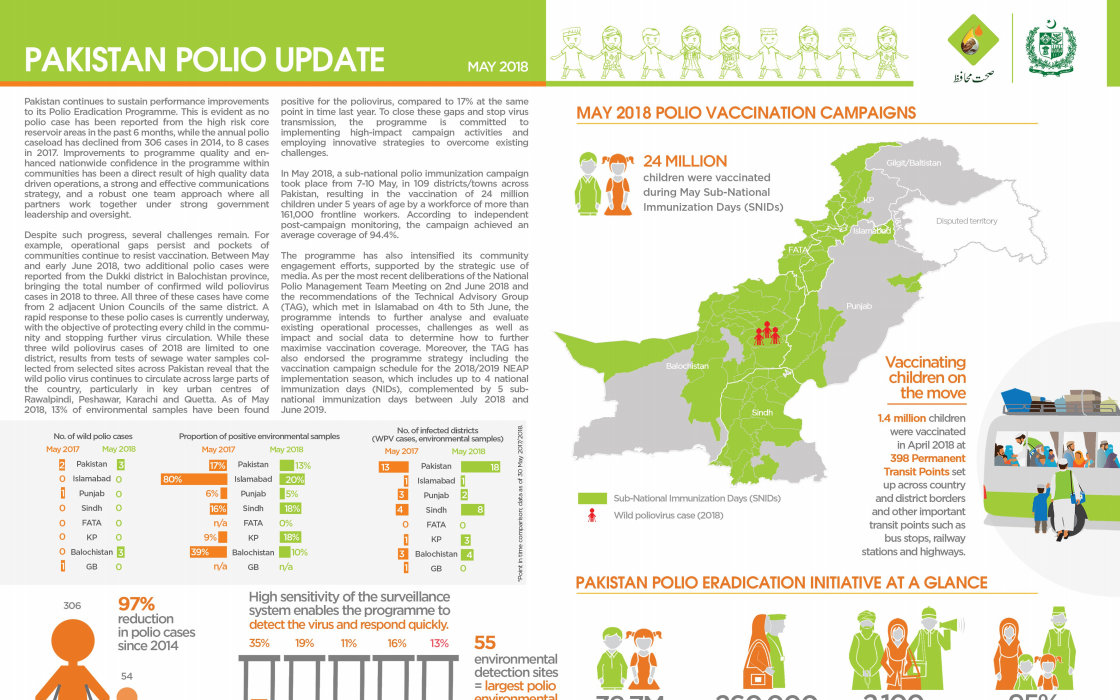
Update on polio eradication efforts in Pakistan for May 2018
Government launches emergency measures to prevent children from lifelong paralysis.
Honorine Mollard Billard, Polio Eradication Officer at WHO, speaks to us about critical country support to vaccination campaigns in Lao PDR...
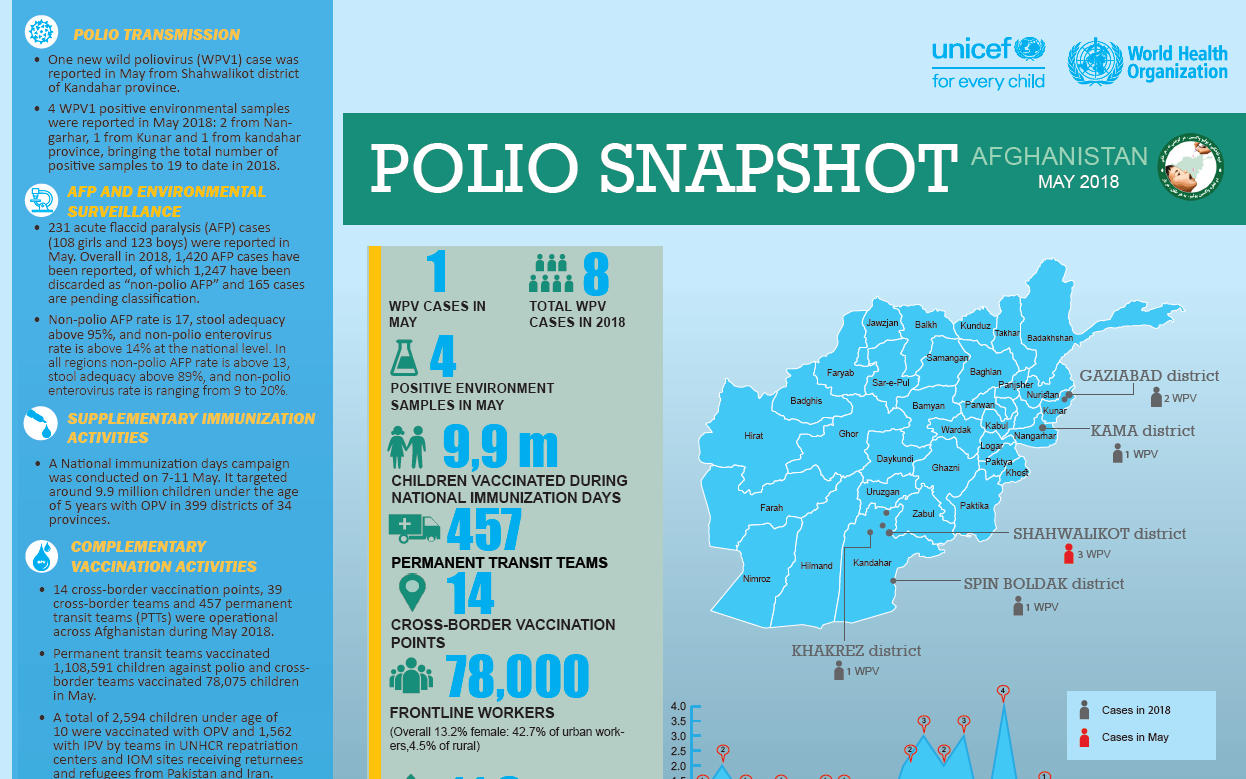
Update on polio eradication efforts in Afghanistan for May 2018
In the sahel surrounding Lake Chad, health workers provide vaccines to refugees and internally displaced people.
In hard-to-reach communities, a Canada-funded project is opening up access to health.
Dr Farzia Sadat was forced out of university for six years, but she persisted. Now she manages over a thousand people in the polio eradicati...
Protecting refugees, returnees and other travelers from the poliovirus is a full-time job along the Afghanistan-Pakistan border.
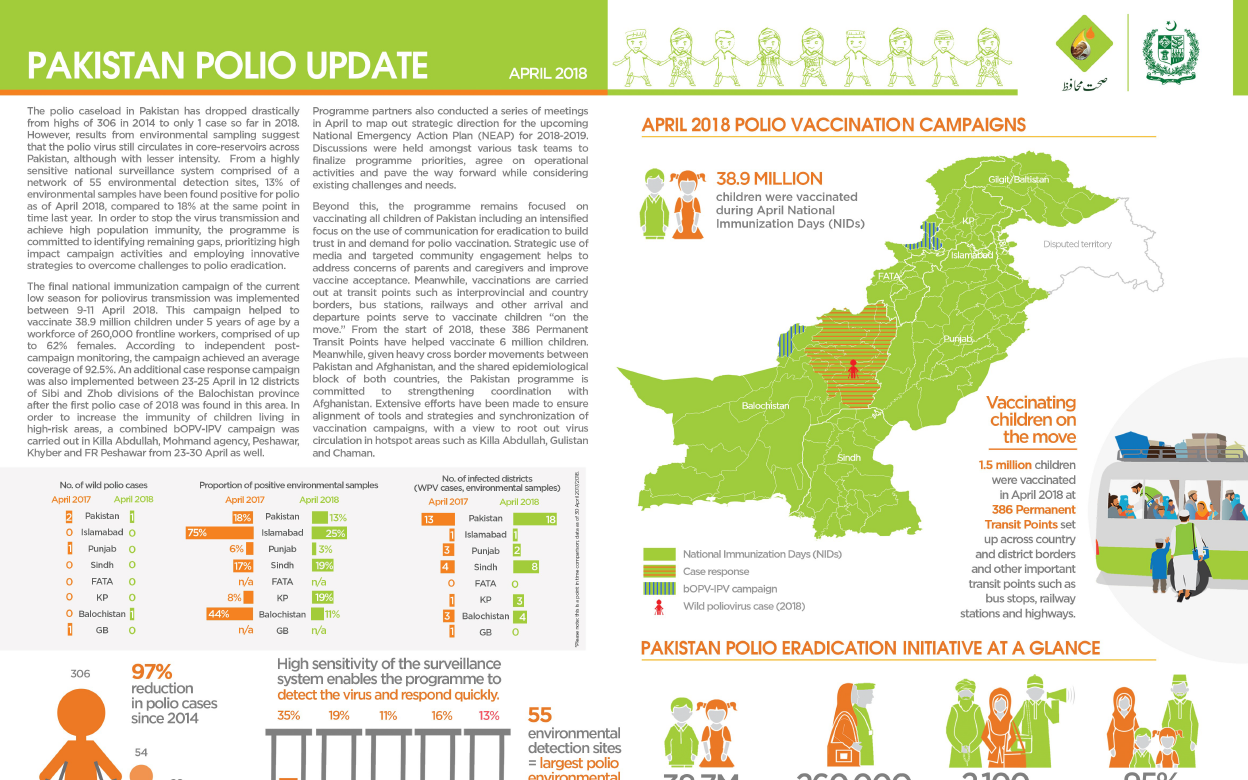
Update on polio eradication efforts in Pakistan for April 2018
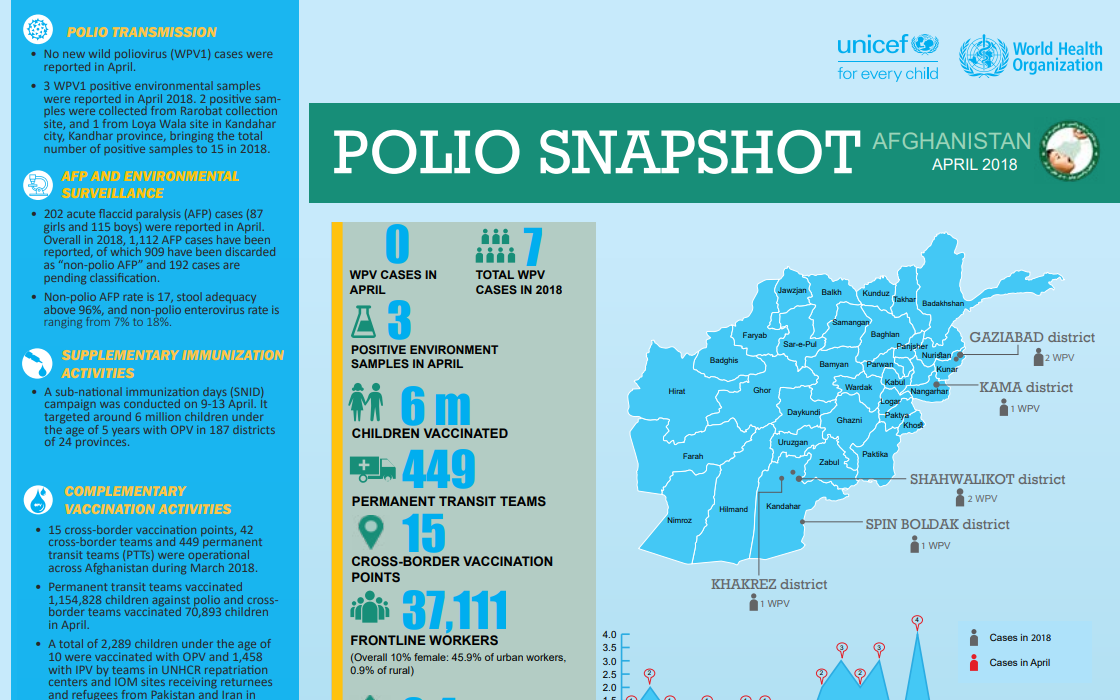
Update on polio eradication efforts in Afghanistan for April 2018
Meet a doctor at the frontline of polio eradication
Immunizing every child in remote communities is a top priority for vaccinators like Daeng
How do vaccinators ensure that every child is reached?
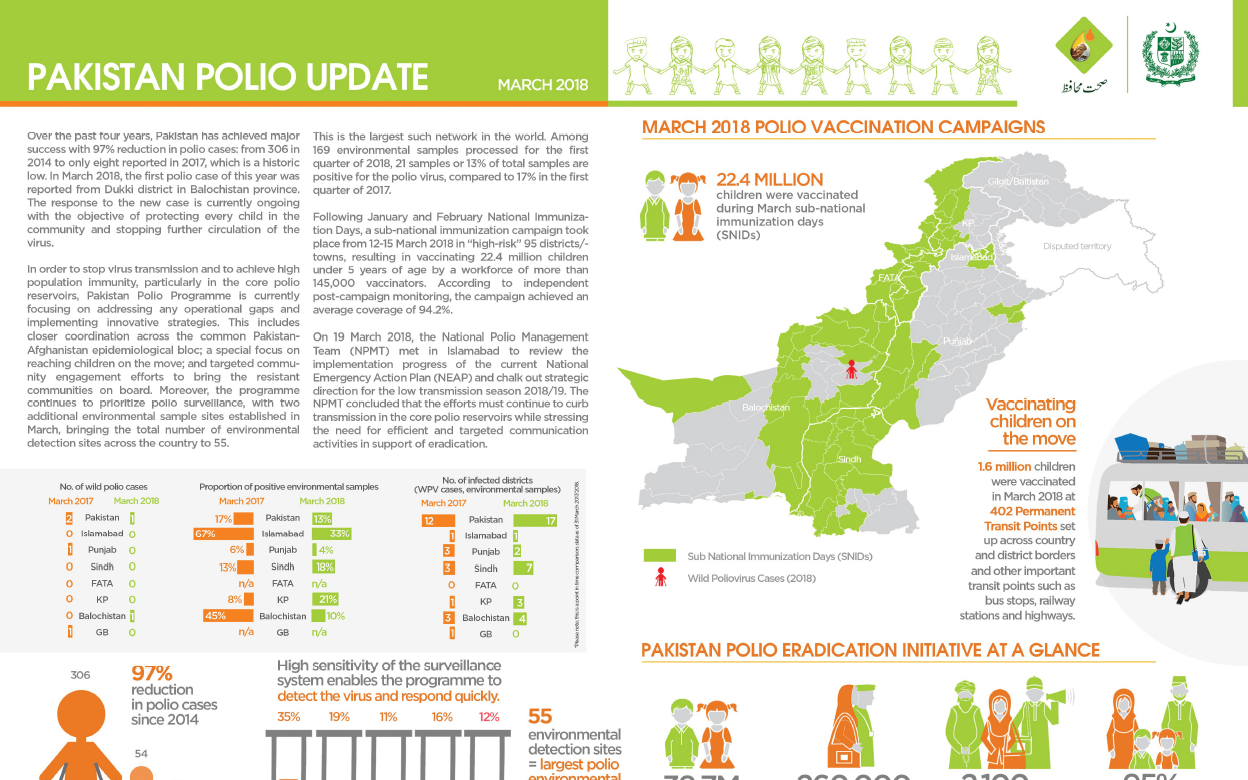
Update on polio eradication efforts in Pakistan for March 2018
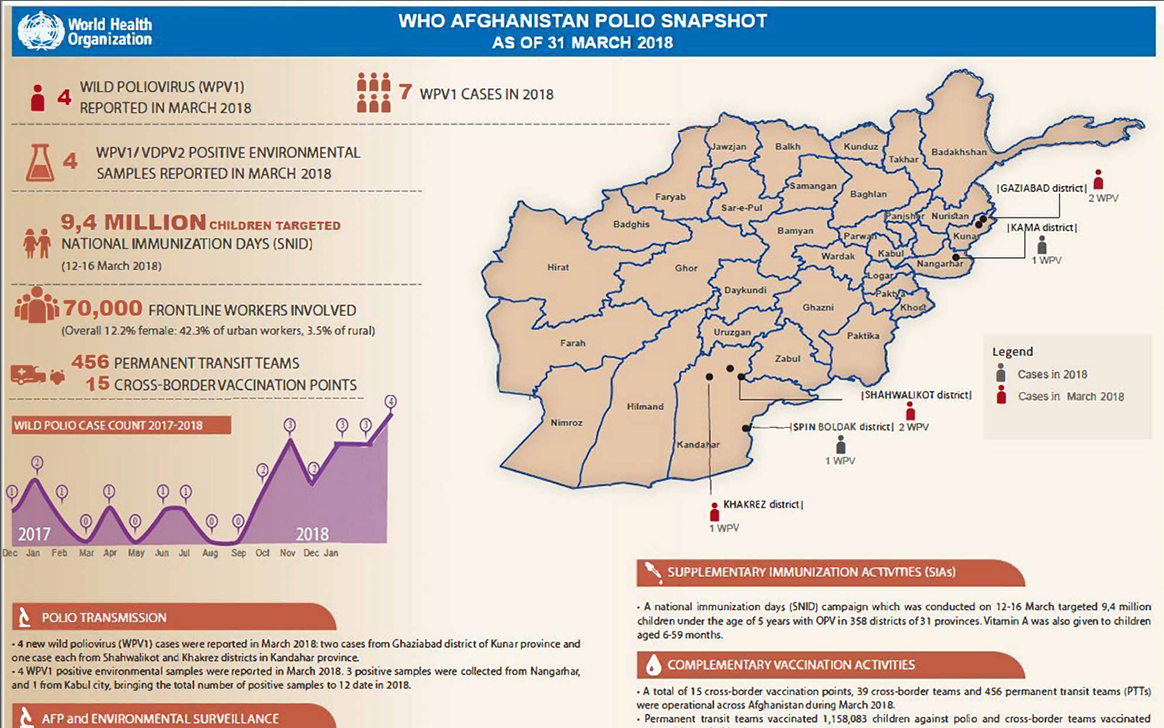
Update on polio eradication efforts in Afghanistan for March 2018
This World Immunization Week, let’s take a few moments to remember what our world really looked like before vaccines.
In Iraq, polio vaccinators work to protect conflict-affected children.
Working with the polio programme opens up new opportunities for women and their communities.