Following confirmation of circulating vaccine-derived poliovirus type 2 (cVDPV2) on 8 January 2019, planning for an outbreak response is und...
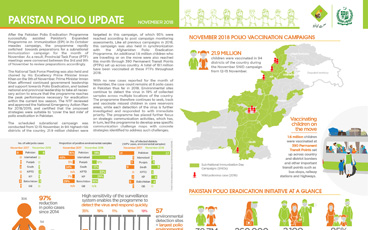
Update on polio eradication efforts in Pakistan for November 2018
In the Horn of Africa polio outbreak, immunization efforts are focusing on a group known as “special populations”.
Early analysis of campaign data points to a successful vaccination round in a polio-free country at risk of possible importation.
To truly ensure no child is left behind, the Global Polio Eradication Initiative is reaching out to some of the most remote communities in t...
Mohamed Shire, a polio eradication expert from Somalia, speaks about lessons from a life tirelessly working to eradicate first smallpox, the...
After an 18-month long intensive vaccination campaign in the face of a poliovirus outbreak in Syria, the outbreak has been successfully stop...
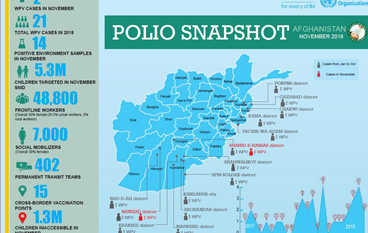
Update on polio eradication efforts in Afghanistan for November 2018
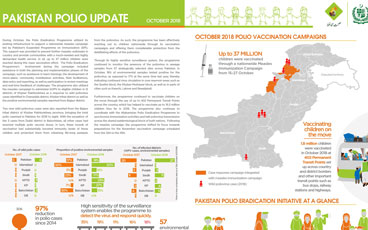
Update on polio eradication efforts in Pakistan for October 2018
Afghanistan aims to reach the most vulnerable in Southern and Eastern provinces.
Dr Zubair Wadood, senior polio epidemiologist and technical expert at WHO, speaks to us about the remaining operational challenges to reachi...
What did we learn?
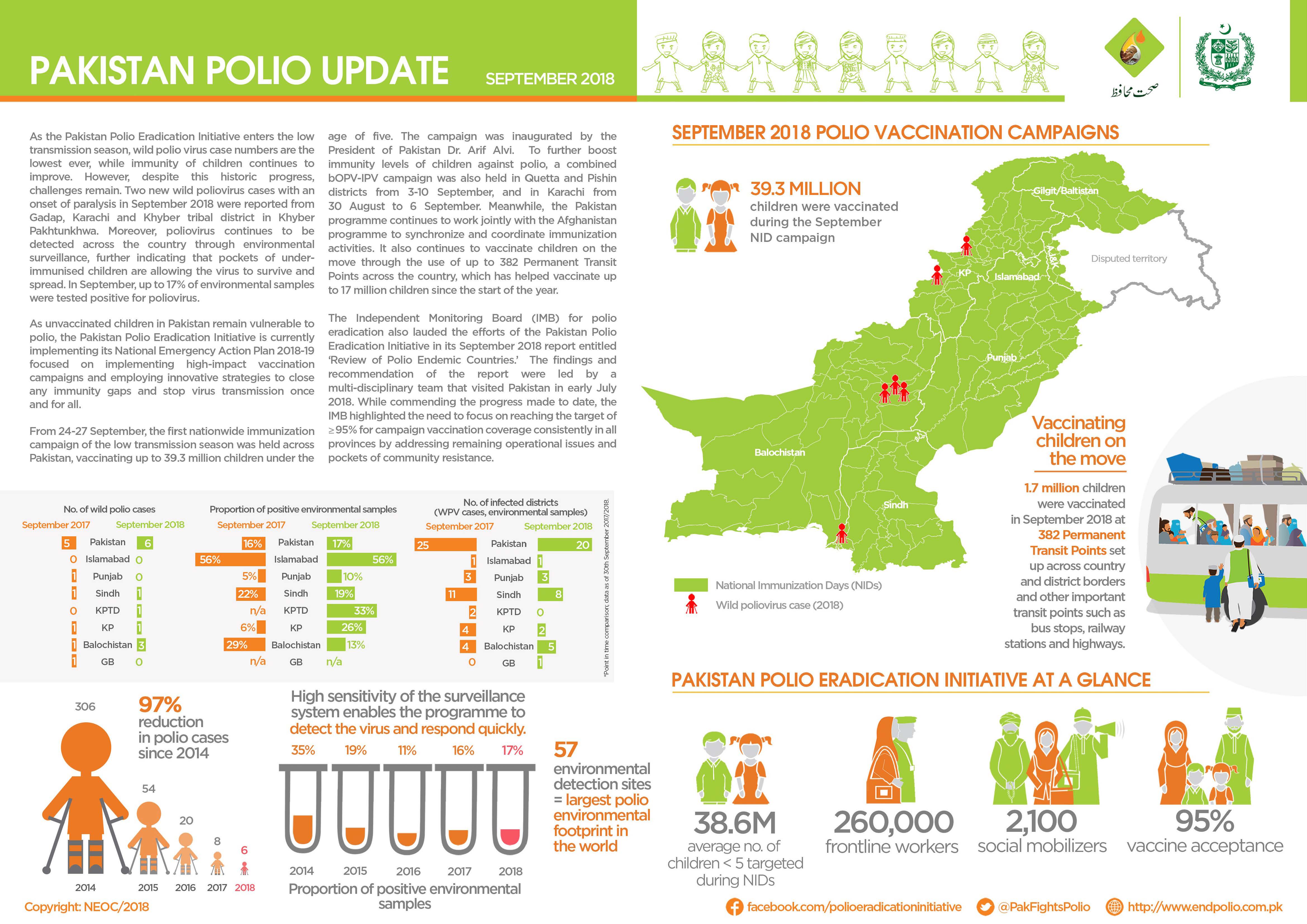
Update on polio eradication efforts in Pakistan for September 2018
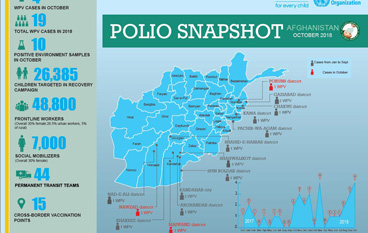
Update on polio eradication efforts in Afghanistan for October 2018
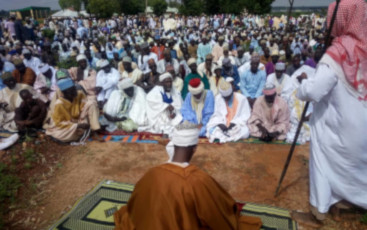
Religious clerics promote routine immunization and other health services by delivering messages to husbands, fathers and sons at mosques.
Over 31 million children will be vaccinated against measles in Pakistan in a countrywide immunization campaign supported by the polio progra...
Special report on Papua New Guinea
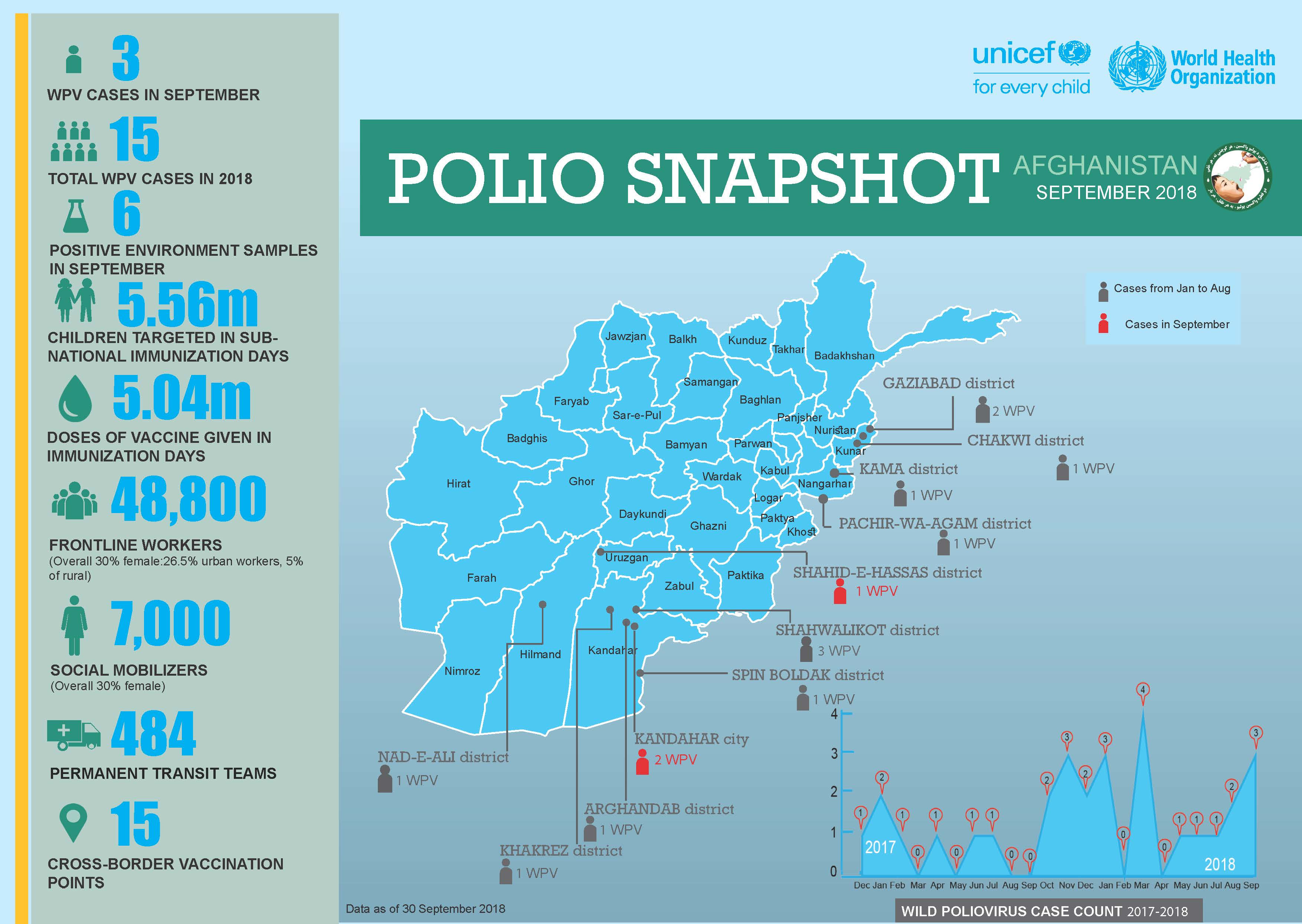
Update on polio eradication efforts in Afghanistan for September 2018
Head of WHO Chad Dr Jean-Bosco Ndihokubwayo speaks about the ongoing efforts to reach every child with polio vaccine across Chad
Meet a religious leader helping to end polio in Pakistan.
Girl or boy, health workers in Nigeria are determined to show parents that the polio vaccination is for all children.
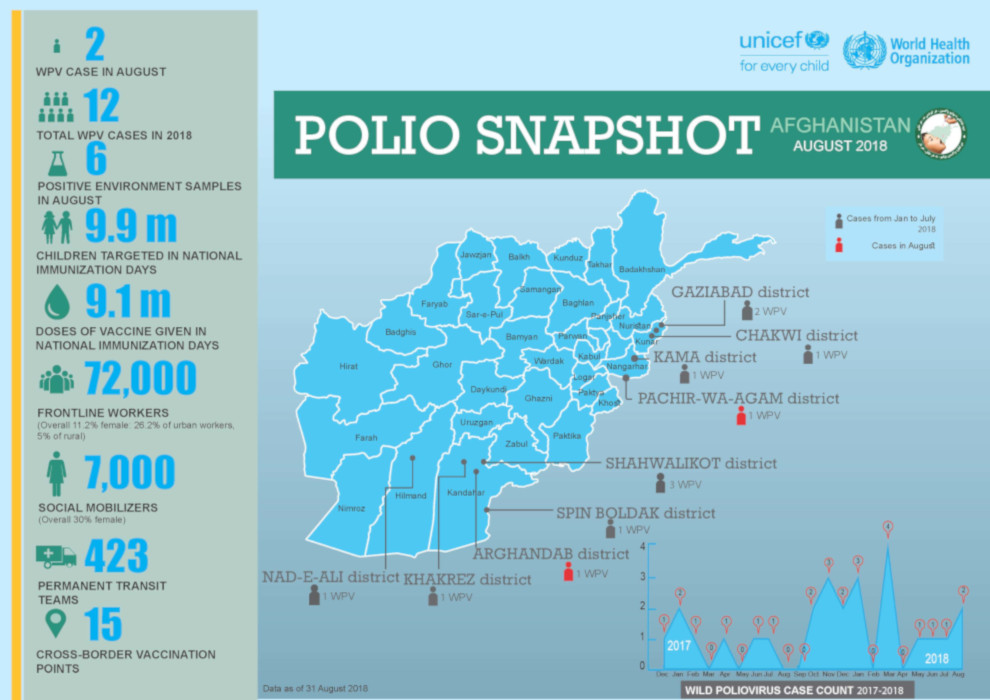
Update on polio eradication efforts in Afghanistan for August 2018
In a complex environment, partners of the polio programme are working to vaccinate every child.
Darcy Levison, WHO Polio Eradication Officer, speaks to us about the logistical challenges of reaching every single child with polio vaccine...
Meet WHO’s Chris Maher, who has spent 25 years following polio to its last hiding places.