Amid geopolitical tensions and insecurity across the Region, health workers in Pakistan and Afghanistan came together in April in a synchron...
New national immunization coverage data released by the World Health Organization (WHO) and UNICEF.
Polio campaign in Gaza Strip reaches around 603 000 children with better access - Joint statement from WHO and UNICEF
Joint statement from WHO and UNICEF
Across Afghanistan, community advocacy to increase vaccine uptake for polio and other deadly diseases has some unsung champions: the local w...
11 March 2024
A polio survivor in Nangarhar shares his challenges and advises parents to vaccinate their children
Making the arduous journeys that underpin Yemen’s effort to end its poliovirus outbreak
22 September 2023
From the field: polio vaccination campaign in Pakistan
Pakistan’s polio program has launched a novel initiative to reach children of nomadic families with polio and essential vaccines so that the...
Qatar, supported by WHO, ramps up surveillance for polio during the FIFA World Cup 2022
1 March 2022
cVDPV2 outbreak response continues in the country
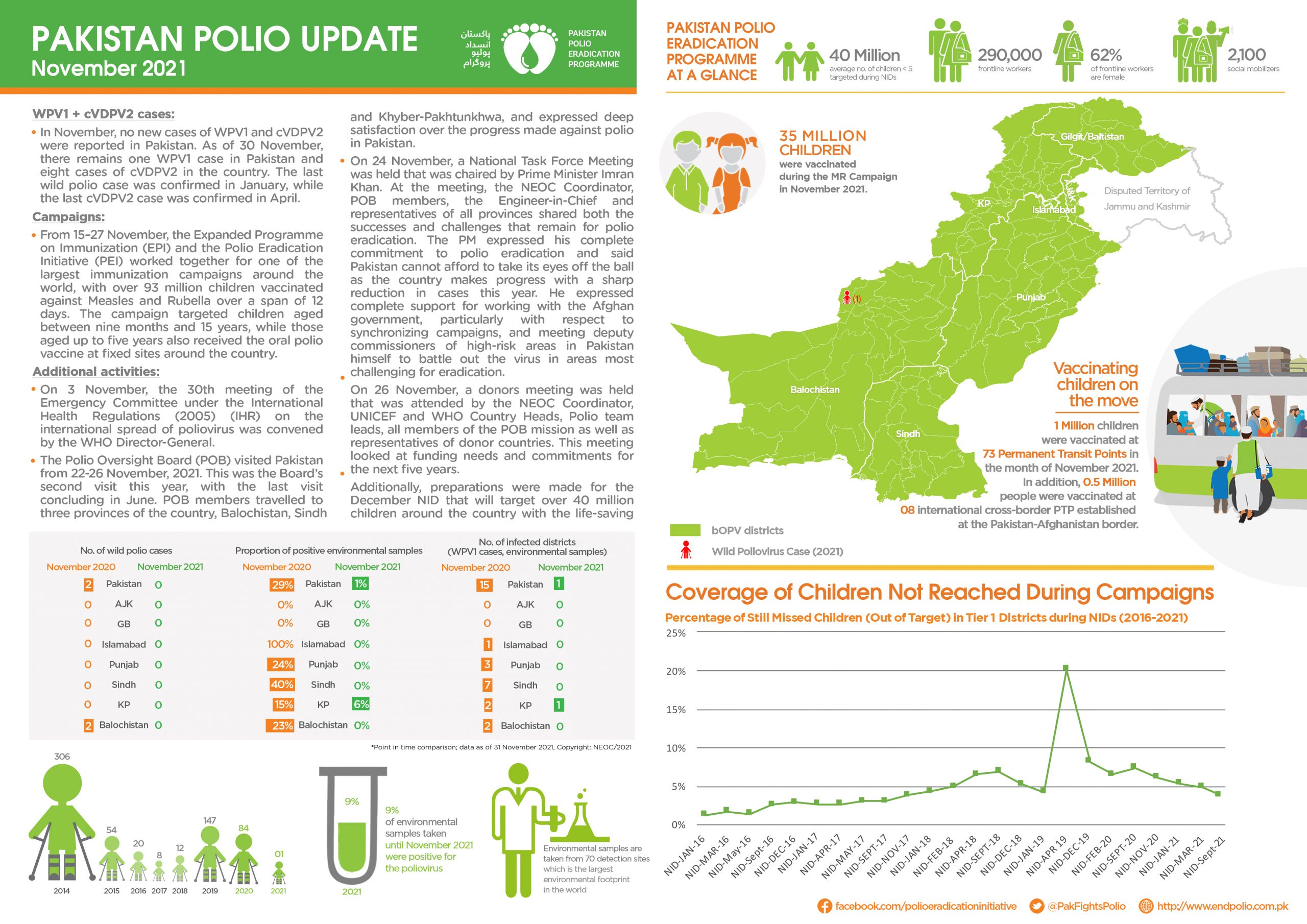
Update on polio eradication efforts in Pakistan for November 2021
Update on polio eradication efforts in Pakistan for October 2021
Polio returned to Tajikistan last year when a circulating vaccine-derived poliovirus type 2 (cVDPV2) outbreak was declared in the province o...
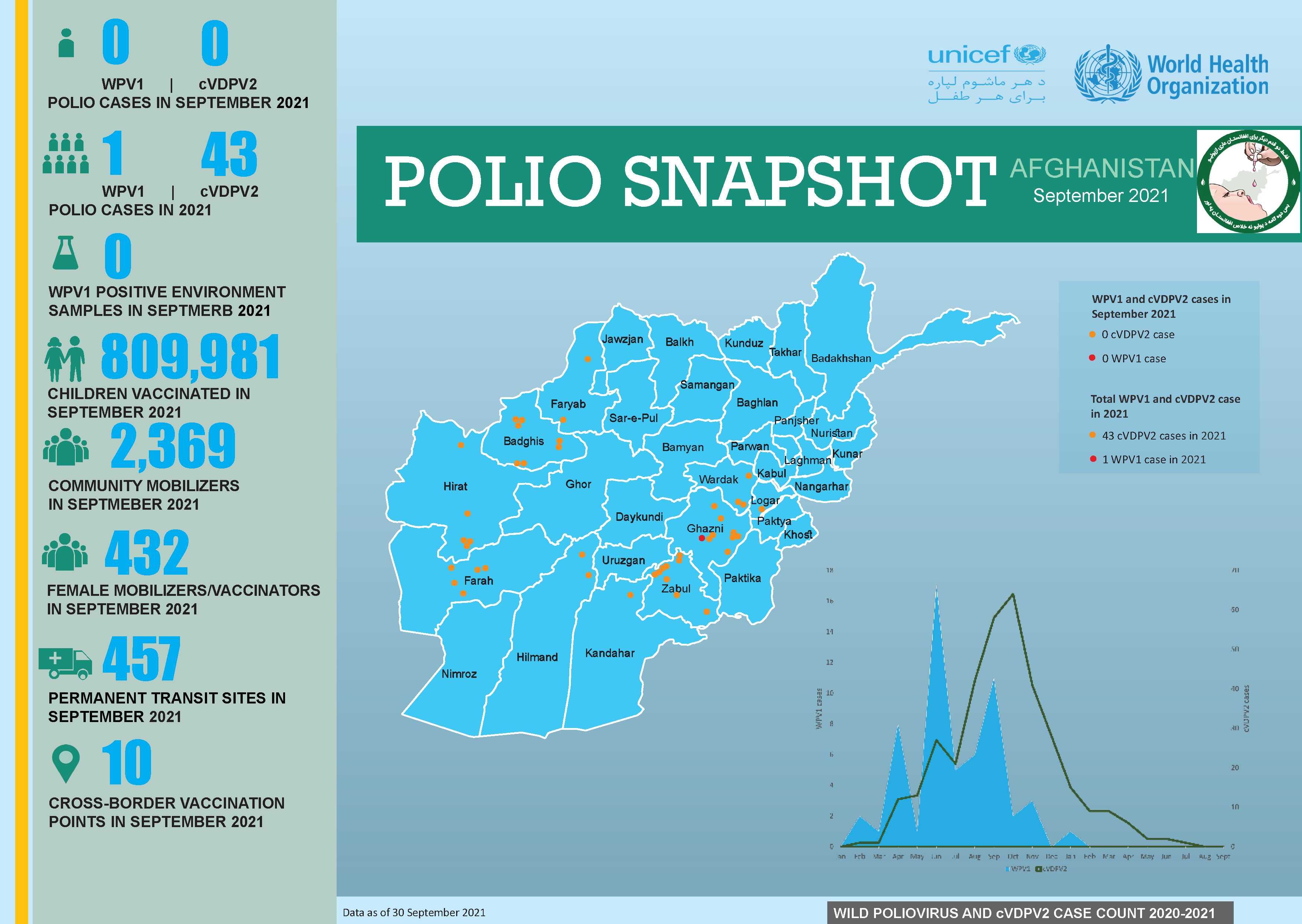
Update on polio eradication efforts in Afghanistan for September 2021
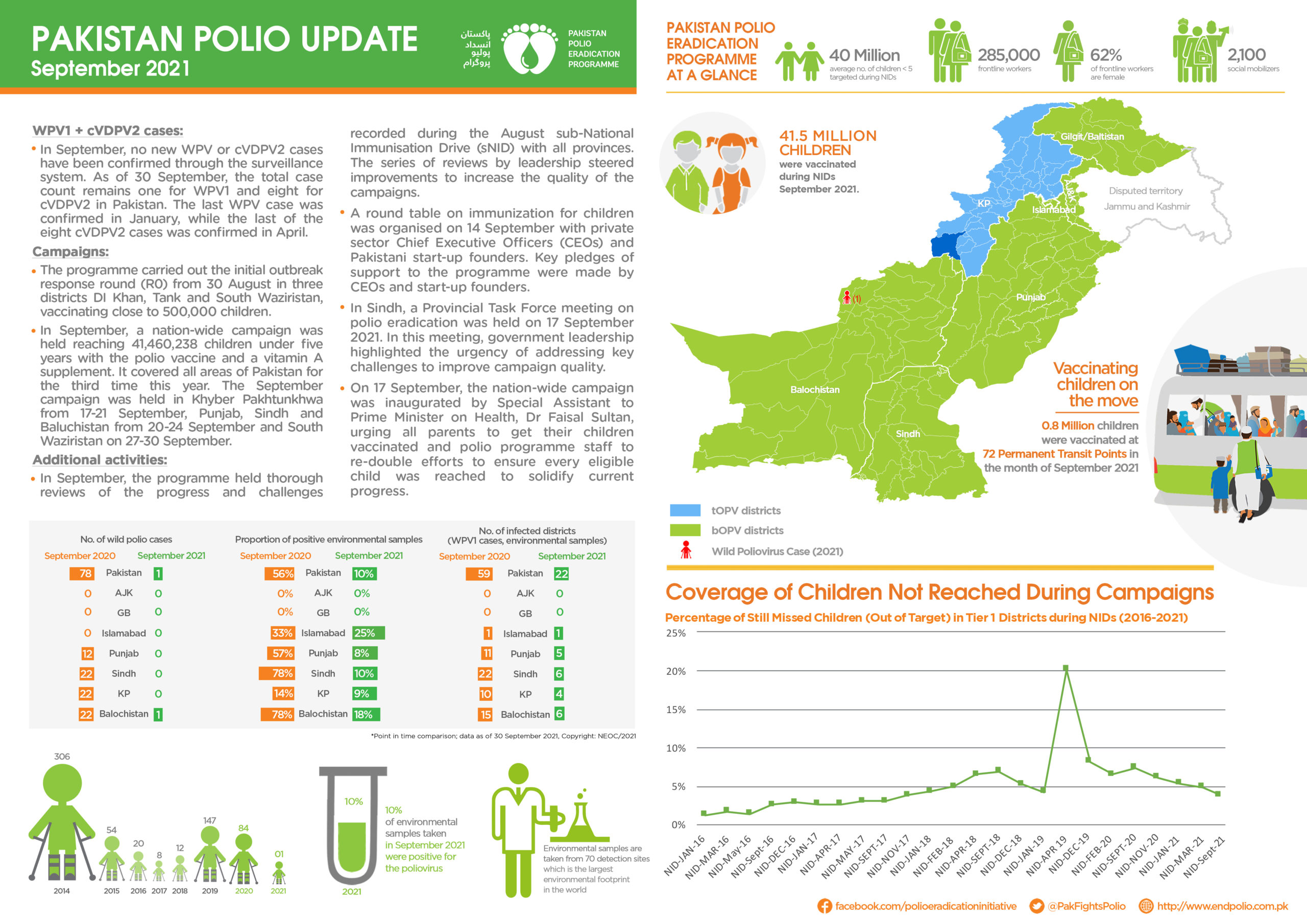
Update on polio eradication efforts in Pakistan for September 2021