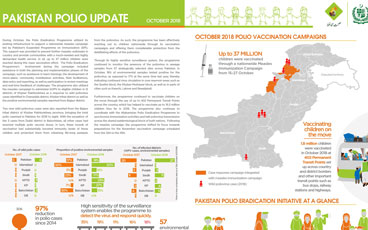
Update on polio eradication efforts in Pakistan for October 2018
Afghanistan aims to reach the most vulnerable in Southern and Eastern provinces.
Dr Zubair Wadood, senior polio epidemiologist and technical expert at WHO, speaks to us about the remaining operational challenges to reachi...
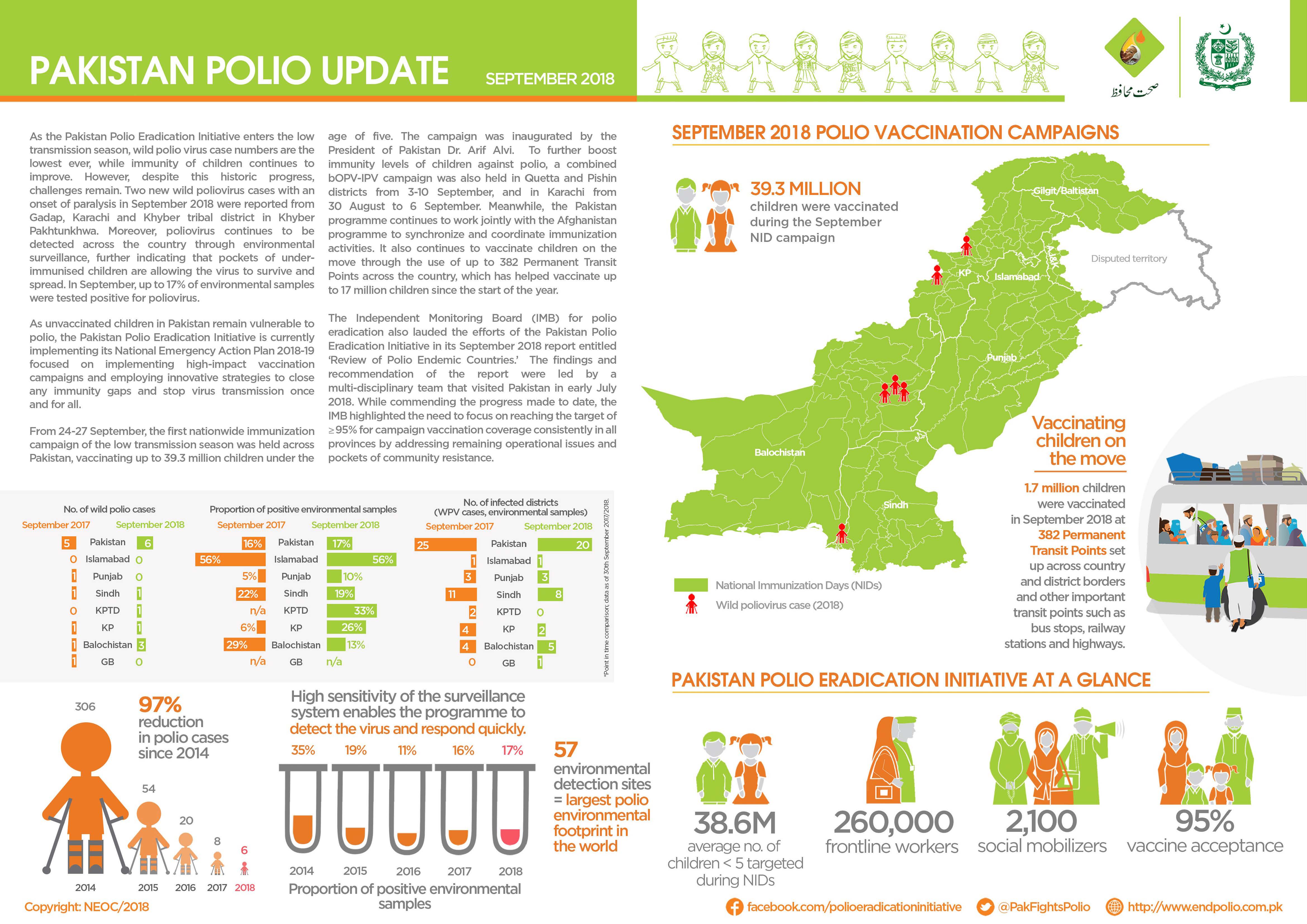
Update on polio eradication efforts in Pakistan for September 2018
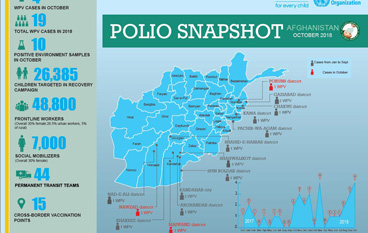
Update on polio eradication efforts in Afghanistan for October 2018
Over 31 million children will be vaccinated against measles in Pakistan in a countrywide immunization campaign supported by the polio progra...
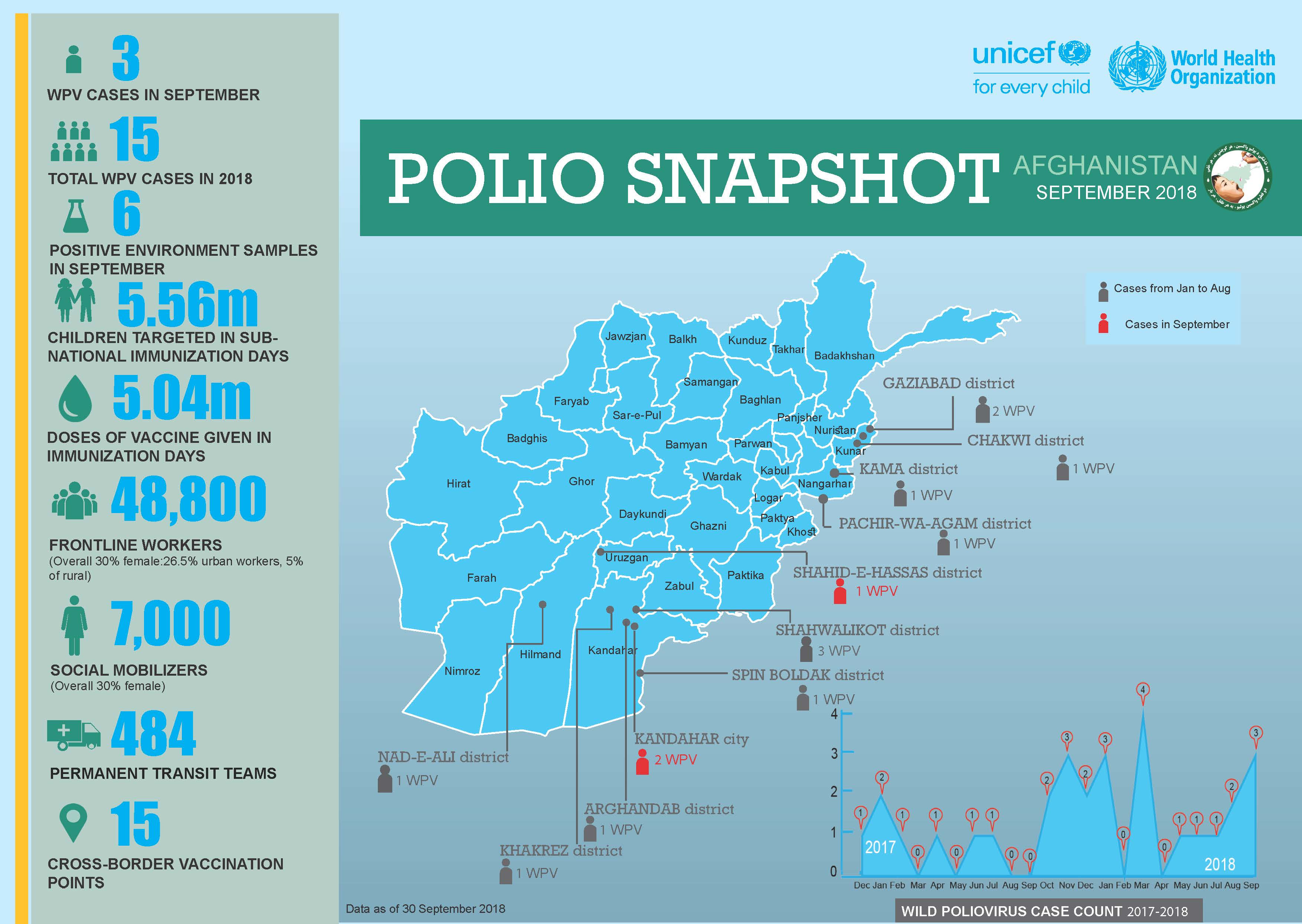
Update on polio eradication efforts in Afghanistan for September 2018
Girl or boy, health workers in Nigeria are determined to show parents that the polio vaccination is for all children.
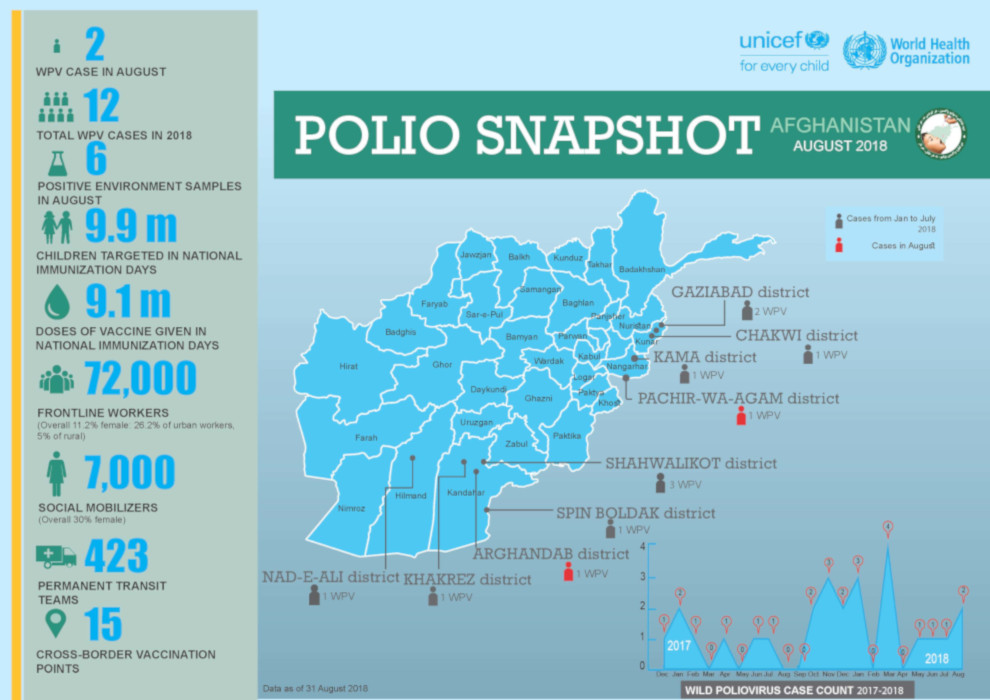
Update on polio eradication efforts in Afghanistan for August 2018
Meet WHO’s Chris Maher, who has spent 25 years following polio to its last hiding places.
On Pakistan Independence Day, vaccinators break records for the number of children protected against polio.
UNICEF community mobilizers engage mothers and fathers to ensure that every child is safe from polio.
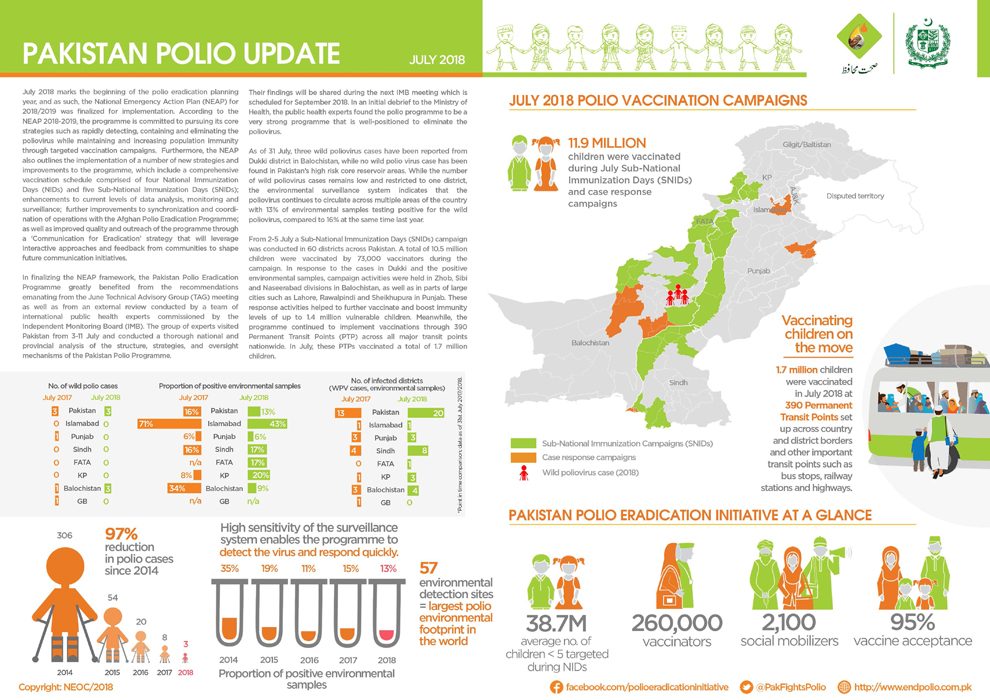
Update on polio eradication efforts in Pakistan for July 2018
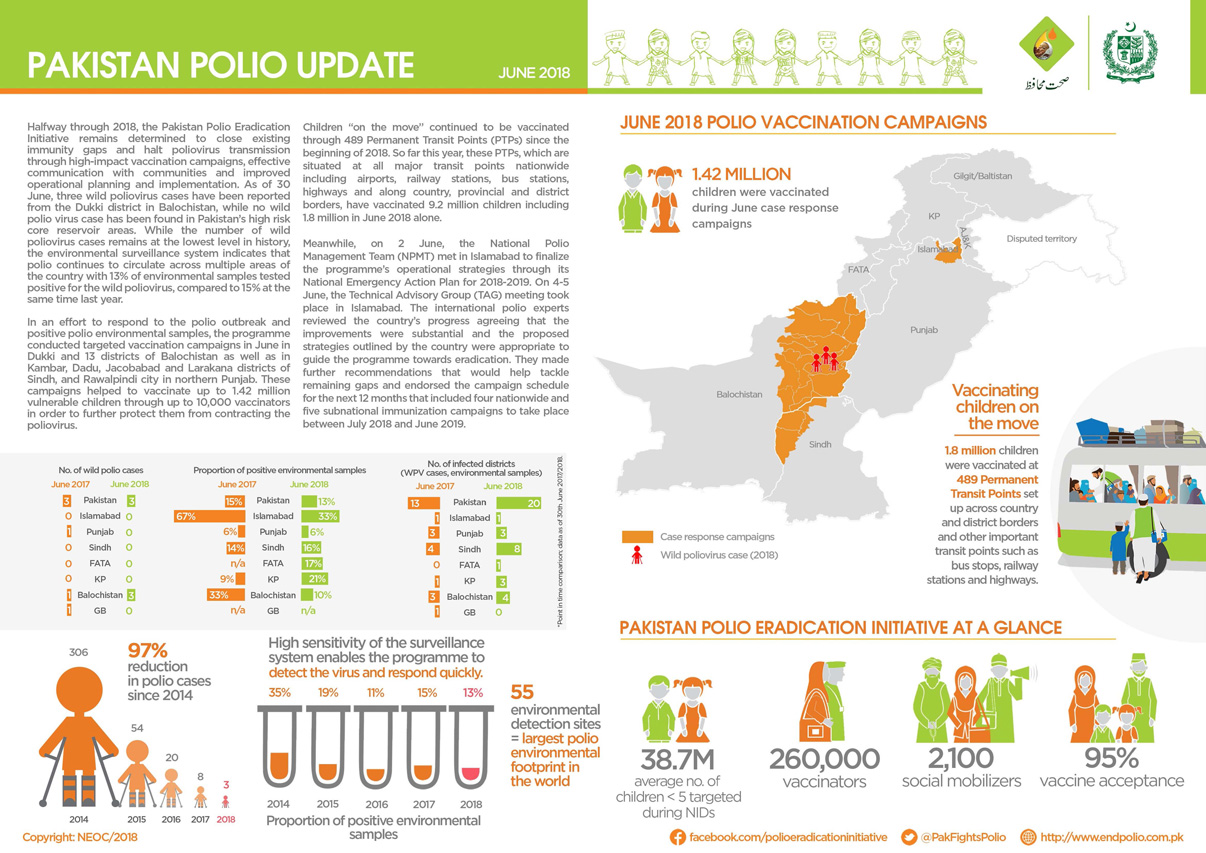
Update on polio eradication efforts in Pakistan for June 2018
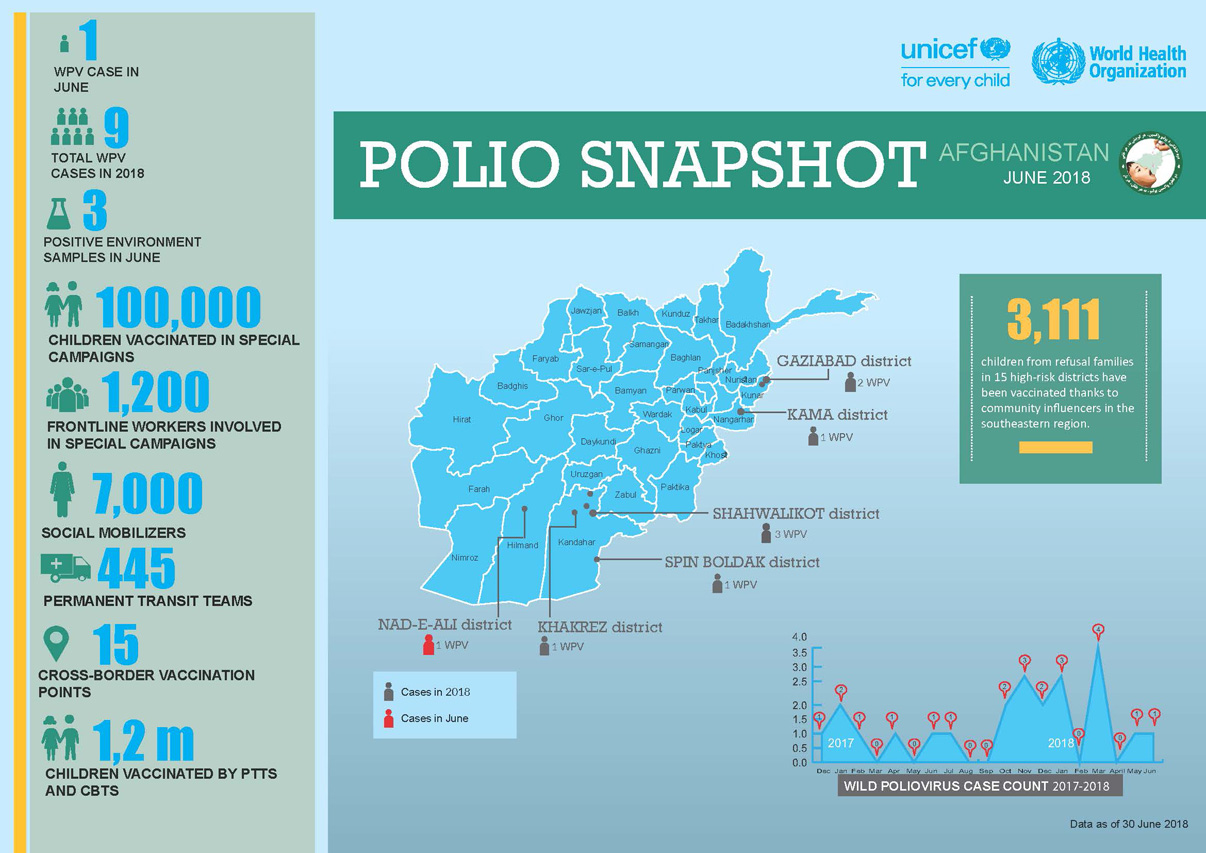
Update on polio eradication efforts in Afghanistan for June 2018
Afia is part of one of the biggest female work forces in Afghanistan.
Across the Lake Chad Basin, e-Surve technology is revolutionizing the way that the polio programme conducts disease surveillance
How a vaccine refuser became an advocate for polio eradication.
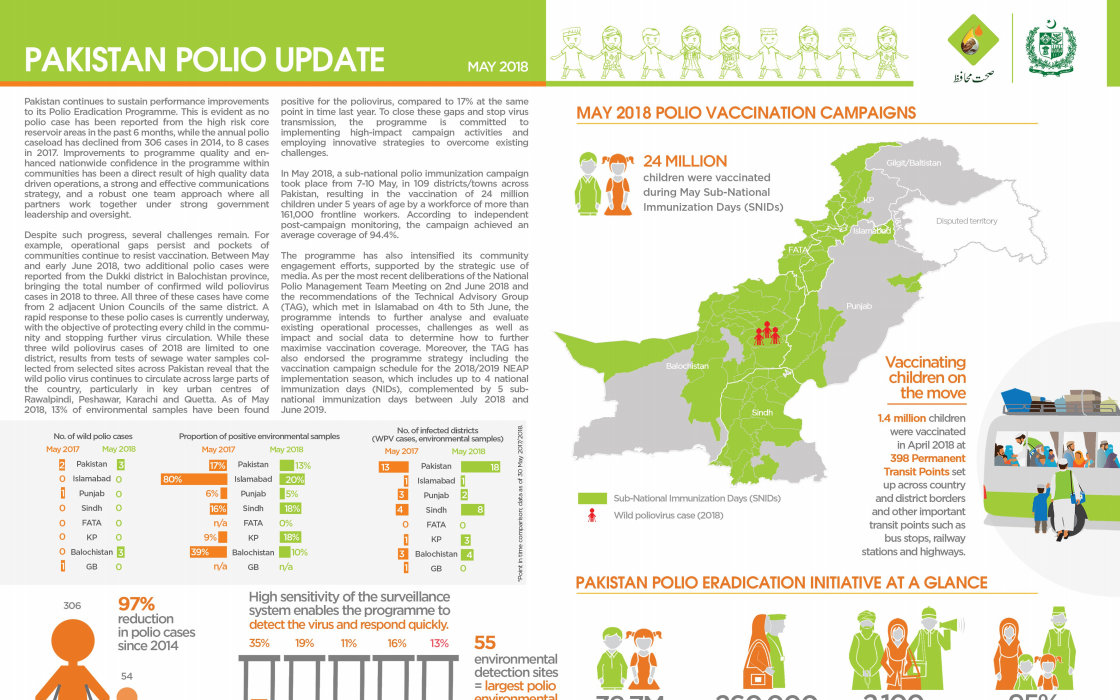
Update on polio eradication efforts in Pakistan for May 2018
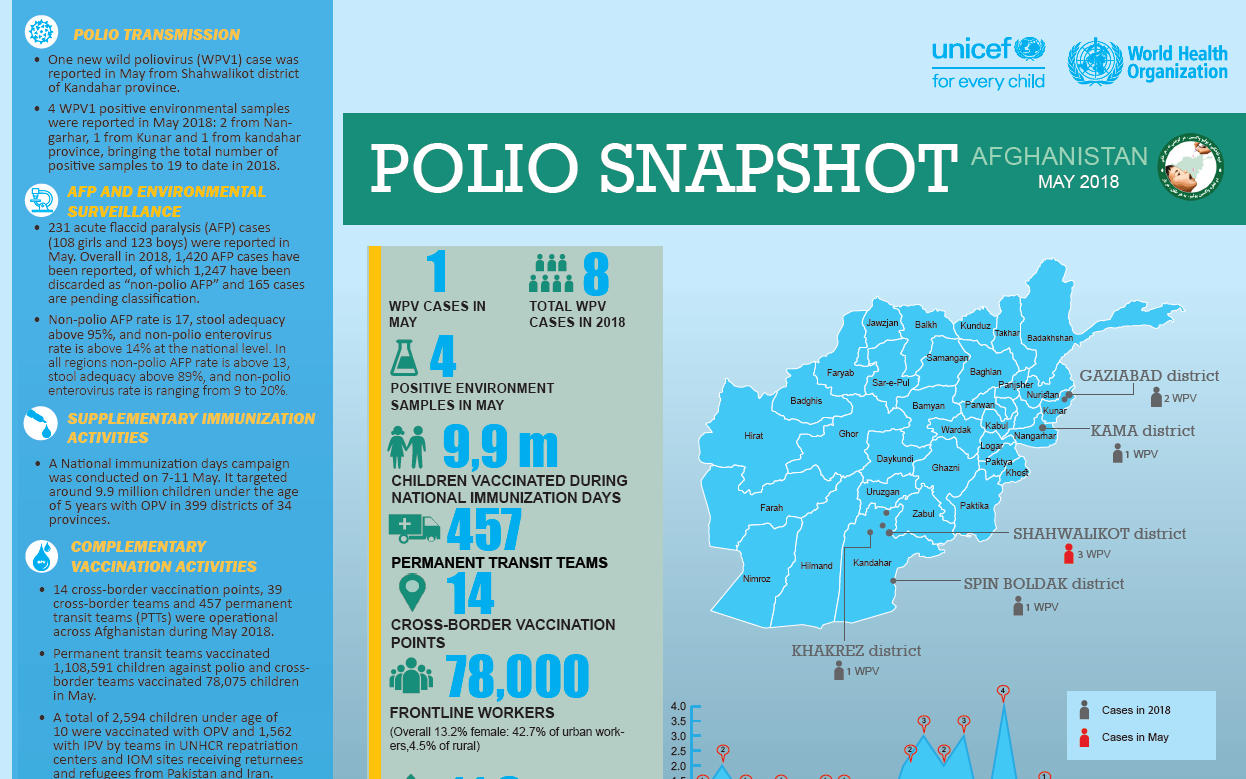
Update on polio eradication efforts in Afghanistan for May 2018
In hard-to-reach communities, a Canada-funded project is opening up access to health.
Dr Farzia Sadat was forced out of university for six years, but she persisted. Now she manages over a thousand people in the polio eradicati...
Protecting refugees, returnees and other travelers from the poliovirus is a full-time job along the Afghanistan-Pakistan border.
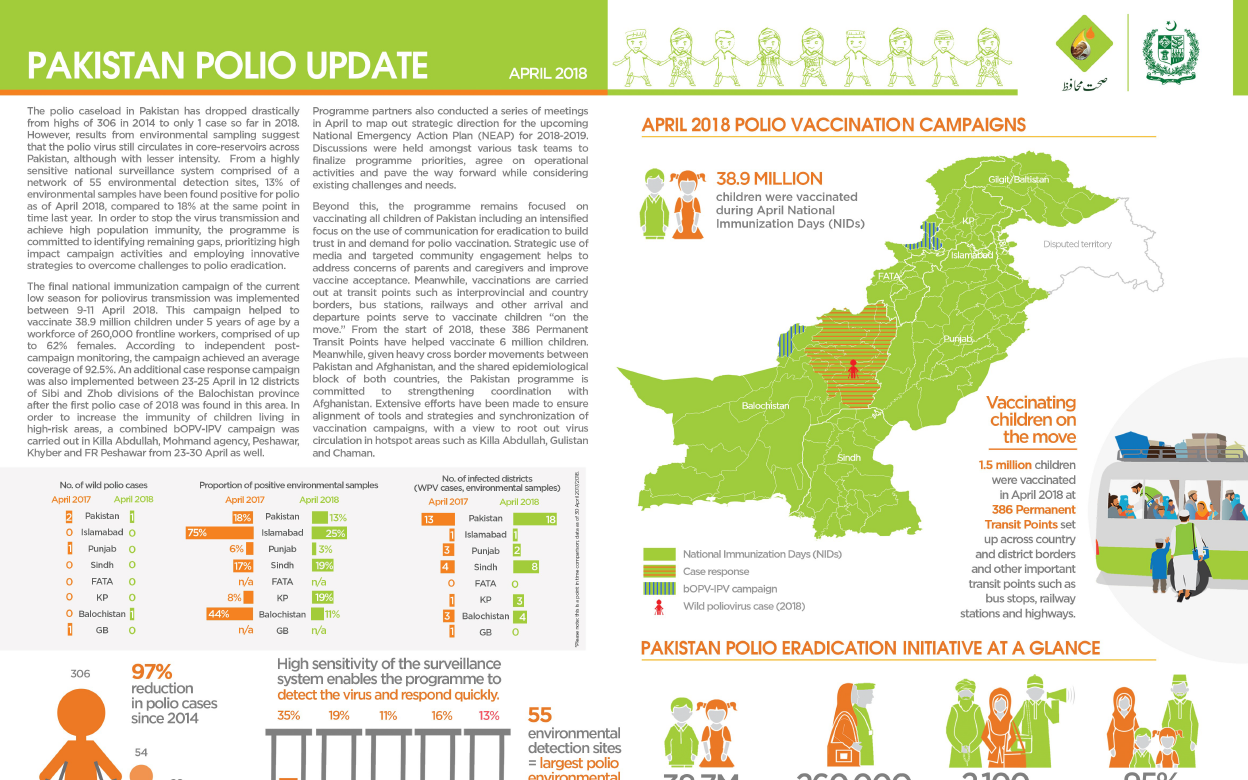
Update on polio eradication efforts in Pakistan for April 2018
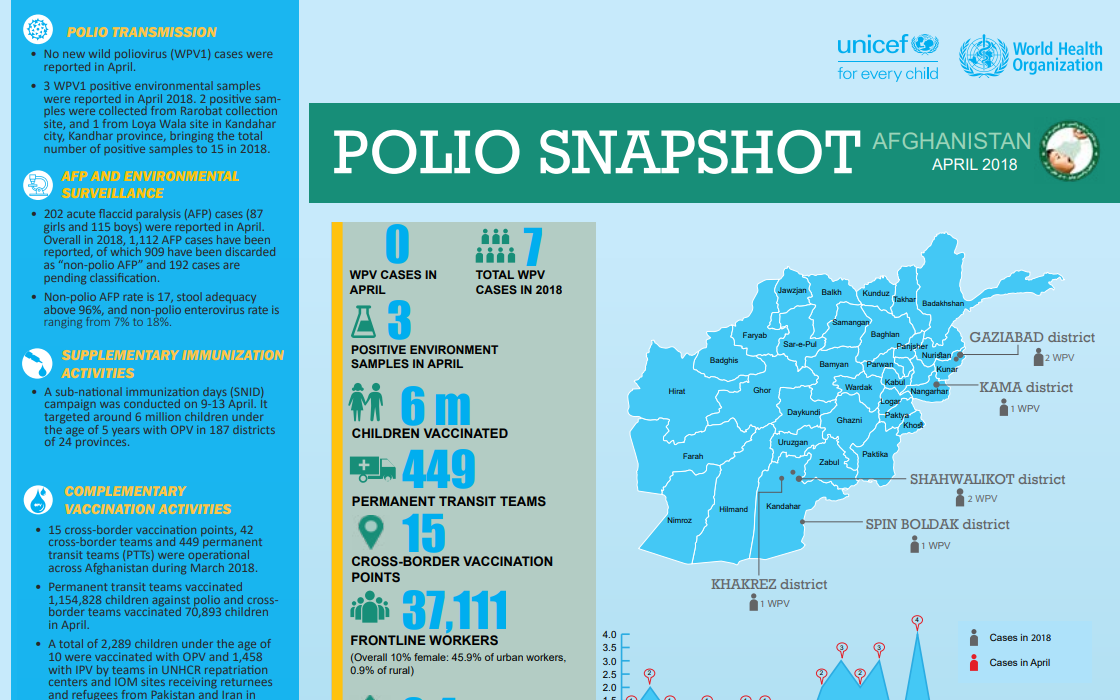
Update on polio eradication efforts in Afghanistan for April 2018