With the global polio case count at the lowest in history, there has never been a better time to invest in surveillance for poliovirus.
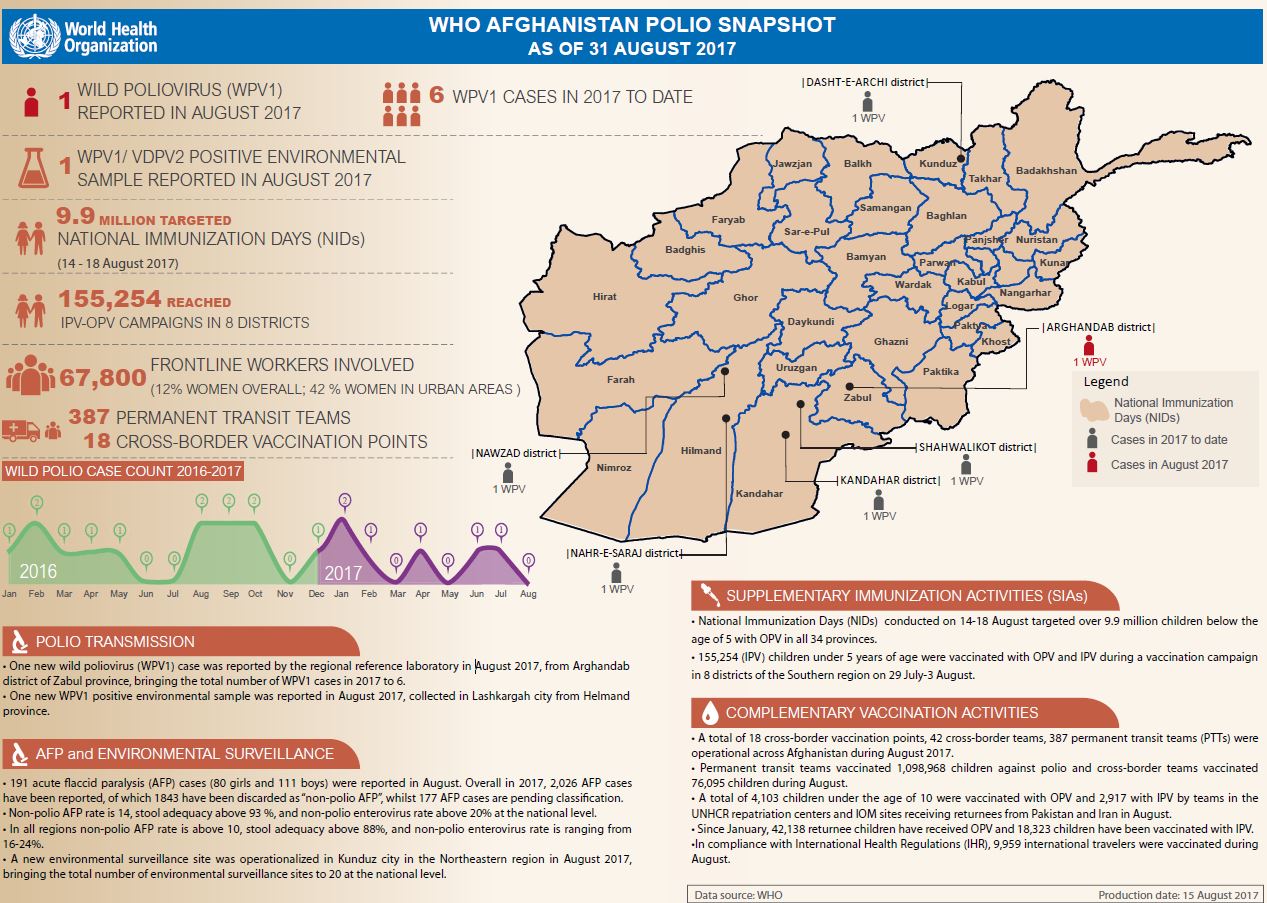
Update on polio eradication efforts in Afghanistan for August 2017
Polio has not been detected for a year, but that doesn't mean it’s gone
On his motorbike, Mullah Rashid criss-crosses Kandahar, talking to communities about the importance of vaccination
Adding creativity and colour to polio eradication efforts in Afghanistan.
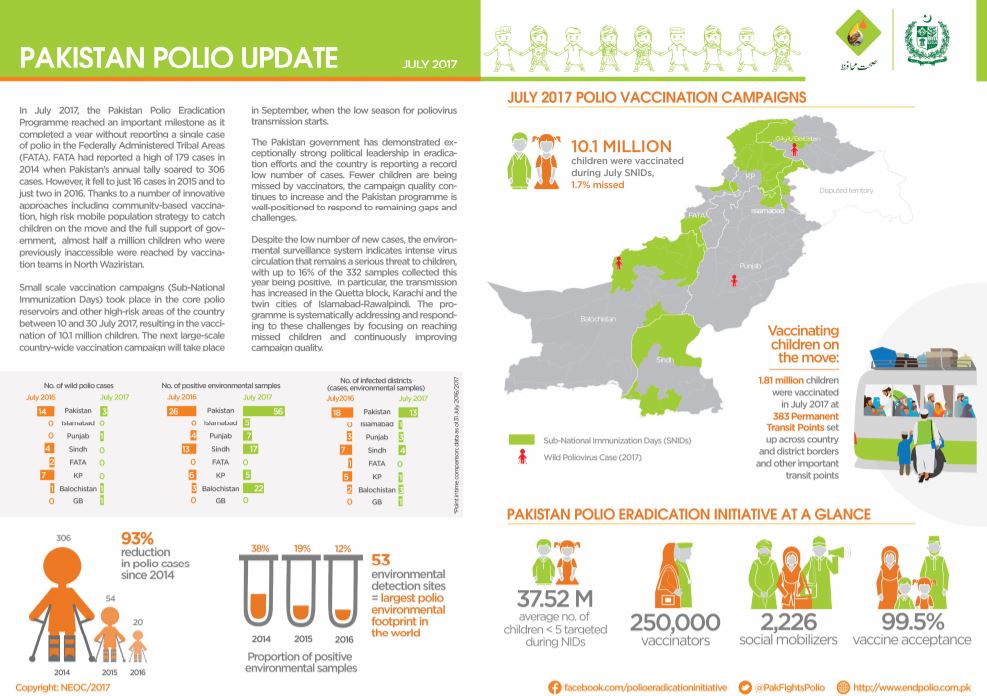
Snapshot of polio eradication efforts in Pakistan for July 2017
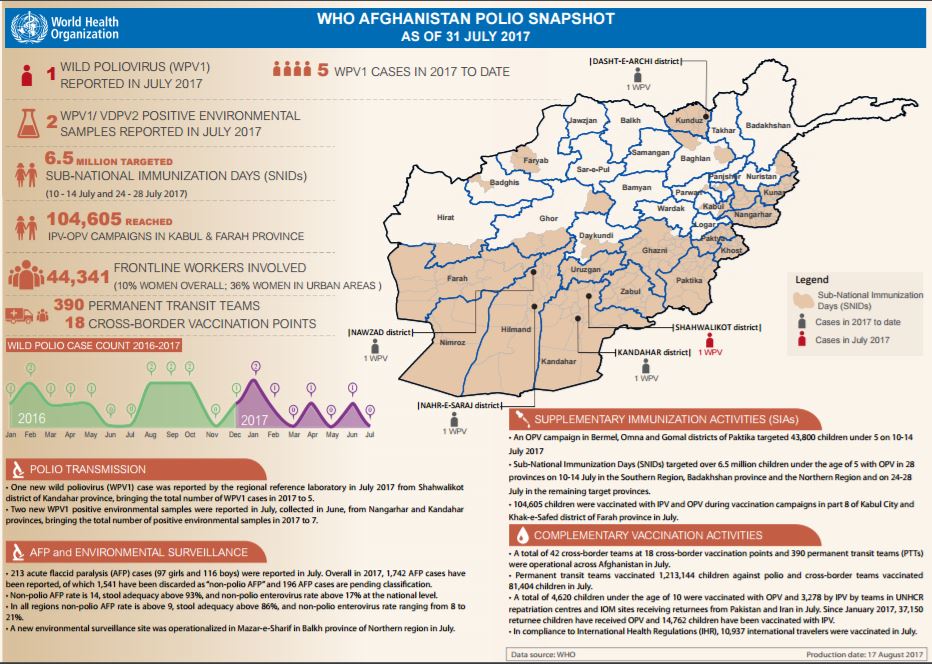
Update on polio eradication efforts in Afghanistan for July 2017
Karachi’s Khalida - forging a path to trust in vaccines
With five national campaigns since October 2016, Pakistan is well positioned to face the challenges ahead.
Saudi Arabia has issued health requirements for travellers during the Hajj season
Important lessons on stopping the poliovirus in the most challenging locations are moving the polio eradication programme closer to the fini...
Countries and partners pledge US$ 1.2 billion to protect 450 million children from polio every year
How Nigeria’s Volunteer Community Mobilizers are delivering more than just polio vaccines
With eradication closer than ever, delegates to the World Health Assembly discussed how to finish the job and address the challenges of the...
Polio staff in Nigeria have contributed emergency response expertise in Sokoto State
116 million children to be immunized from coast to coast across the continent, as regional emergency outbreak response intensifies
Meet the Afghan women helping to bring the world closer to eradication
Afghanistan steps up surveillance to accelerate polio eradication
A €70 million EU grant will support polio eradication and efforts and health systems strengthening in Nigeria
Afghanistan’s determined effort to end polio
Afghanistan is reaching over 5.6 million children with vaccines against polio during large-scale campaign starting in January.
Ministries of health from around the world call for urgent measures to secure lasting polio-free world
Tahera and over 65,000 dedicated frontline workers are at the heart of efforts to eradicate polio from Afghanistan.
In January, the polio programme is contributing to the protection of more than 4 million children against measles.
Meet the frontline health workers and community mobilizers who are striving to reach and protect some of the world’s most vulnerable childre...