Seventh meeting of the Regional Subcommittee for Polio Eradication and Outbreaks - 28 February 2023
Insecurity and displacement increase risk of diseases such as polio
“I hope one day I can tell my son the story of how polio was eradicated and how no child will ever be paralyzed by this virus again.”
Update on polio eradication efforts in Pakistan for January 2021
Update on polio eradication efforts in Afghanistan for October 2020
Update on polio eradication efforts in Pakistan for September 2020
Polio social mobilisers have adapted their work to support families in Afghanistan.
Kenya, Mozambique and Niger have curbed polio outbreaks that erupted in different episodes over the past 24 months, World Health Organizatio...
Everyday people in Pakistan advocating for vaccinations
Early analysis of campaign data points to a successful vaccination round in a polio-free country at risk of possible importation.
Dr Zubair Wadood, senior polio epidemiologist and technical expert at WHO, speaks to us about the remaining operational challenges to reachi...
UNICEF community mobilizers engage mothers and fathers to ensure that every child is safe from polio.
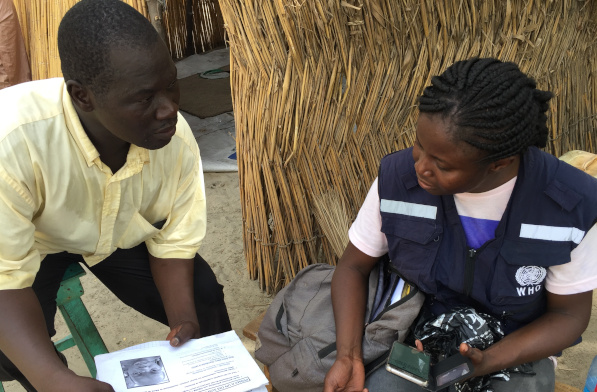
Across the Lake Chad Basin, e-Surve technology is revolutionizing the way that the polio programme conducts disease surveillance
Honorine Mollard Billard, Polio Eradication Officer at WHO, speaks to us about critical country support to vaccination campaigns in Lao PDR...
This World Immunization Week, let’s take a few moments to remember what our world really looked like before vaccines.
In Nigeria, dedicated female mobilizers are critical in the fight against polio.
In at-risk areas of Chad, large-scale polio campaigns are increasing the immunity of every child.
Polio can’t be cured, but it can be prevented. Two important tools help to prevent polio – two safe, effective vaccines. Find out about the...
Hans Everts, long time polio eradicator, shares personal stories from the frontline of outbreak response, and explains how the lessons learn...
Mohammed Mohammedi, country support officer for the Eastern Mediterranean region, speaks to us about the main challenges facing countries an...
We join Dr Urs Herzog, Rotarian, polio eradicator, National PolioPlus Advocacy Advisor for Rotary Switzerland and polio survivor himself, as...
In Pakistan, the polio eradication programme and the routine immunization programme are working hand in hand to increase vaccination coverag...
Different methods of community engagement help to protect every child with vaccines.
In Afghanistan, blood tests are identifying where vaccination campaigns are working, and where gaps remain to be filled.
One of an animated series on the global drive to eradicate polio.