Regional leaders call for intensified support to stop wild poliovirus transmission in Afghanistan and Pakistan
Hamid Jafari talks to Gary Humphreys about the non-linear nature of progress toward polio eradication and the challenges faced in the last t...
The ‘father’ of polio laboratories in the Eastern Mediterranean Region
Seventh meeting of the Regional Subcommittee for Polio Eradication and Outbreaks - 28 February 2023
16 January 2023
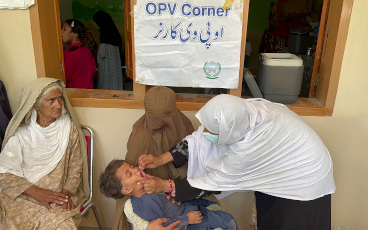
When a mother brought her young son to a clinic in Paghman, a town not far from the Afghan capital Kabul, Spogmai, a nurse on duty at the ti...
Recommendations from the international review of Afghanistan’s poliovirus surveillance system are yielding important results for the country...
As 2022 draws to a close, independent technical bodies from key epi-centres dive deep on what it will take to achieve success in 2023
“Rarely have I seen such commitment and dedication as I have seen in Pakistan.”
One year on from Afghanistan’s transition of power in August 2021, WHO’s polio eradication programme has made critical gains – but the job i...
Polio cases have nose-dived by 99% since the late 1980s after a push to eradicate the disease, but clusters of cases across the world indica...
Rapid action needed to effectively quash transmission
18 May 2022
With wild polio at lowest levels in history, SAGE also turns focus on post-eradication
Polio workers in Afghanistan like Subhania are working hard to protect children against polio and other vaccine preventable diseases.