A unique group of people gathered last month in Sokoto state to commit to the twin goals of eradicating polio, and working to rapidly strengthen routine immunization. Bill Gates, and Africa’s richest man, Alhaji Aliko Dangote, joined traditional leaders from across northern Nigeria, Federal Ministry of Health officials, representatives from several State governments, and partners including UNICEF and WHO.
The two billionaires play a significant role in the fight to eliminate polio in Nigeria, where no wild virus has been detected since 2016. The Bill & Melinda Gates Foundation has committed US$1.6 billion in the country to date to fund pilot projects targeted at health care, agriculture and financial inclusion, a contribution which makes up their biggest investment in Africa. Aliko Dangote, who is Nigerian, has previously worked with Mr Gates to help interrupt transmission of the poliovirus in his country, and helps fund other health programmes as president of the Dangote Foundation.
During their visit, Mr Gates and Mr Dangote witnessed first-hand the progress Nigeria is making in polio eradication, routine immunization and primary health care provision.
At meetings held at the Sultan’s Palace and Governor’s House, Mr Gates highlighted the commitment of traditional leaders and reiterated the importance of engaging communities to reach every child with vaccines. Expressing his concern over the high infant mortality rate in Nigeria, he noted that vaccination is a cost effective way to save children’s lives.
Mr Gates also talked about the need to plan for the future of a polio-free Nigeria. Looking to how the polio eradication infrastructure can be used to help meet other health needs, Mr Gates said that the strong existing polio infrastructure – including vaccine supply chains, disease surveillance, laboratory systems and social mobilization networks – can be used to develop and improve routine immunization coverage for other diseases.
“We can prevent millions of deaths through routine immunization,” Mr Gates said. “We will not relent in our commitment towards this.”
Mr Dangote further highlighted that the fight against polio requires commitment from all stakeholders.
Drawing attention to malnutrition as one of the biggest factors undermining Nigeria’s progress, Mr Dangote urged the government and partners to reach out to private sector companies and ask them to donate at minimum 1% of their profits to financing the health sector.
At the meeting, the governors of Bauchi, Borno, Kebbi, Kaduna, Kano, and Sokoto States signed extensions of their Memorandum of Understanding on routine immunization. In doing so they reaffirmed their commitment to maximizing immunization coverage in their respective states, helping to protect every child against polio and other vaccine-preventable diseases.
“When I received the confirmation of the first case of Lassa fever…nothing prepared me for the tasks ahead other than my work in polio eradication” – Mrs Faith Ireye, WHO State Coordinator in Edo state.
In the first two months of 2018, there were 110 deaths in Nigeria from suspected Lassa fever. Outbreak response, led by the Nigerian government and WHO, is focused on detecting every case, and tracing the virus wherever it is hiding.
Bolstering this effort are individuals with experience of guarding against a different disease – polio.
Ms Ireye, who has worked with the Global Polio Eradication Initiative for over ten years, is currently helping to coordinate the Lassa fever outbreak response in Edo State, one of the hardest hit by the outbreak.
“My experiences in polio eradication activities allowed me to immediately swing into action. So, when the [Lassa fever] outbreak was confirmed, I realized the need to use my expertise to serve communities at risk,” she says.
Part of her job is to help coordinate surveillance, specifically ensuring that everyone who has come into contact with someone with Lassa fever is found, and tested for the virus.
Her work is critical to help prevent further fever cases. Deputy Governor of Edo State, His Excellency Philip Shaibu said, “WHO…is one of the pillars that have helped lead surveillance in Edo state… In this particular outbreak, WHO was the first to draw attention to the fact that we need to galvanize resources from all partners, from other parts of the country, to ensure that things get done.”
The polio infrastructure
When outbreaks of other diseases happen, the knowledge and experience of polio personnel like Ms Ireye can make a significant difference to outbreak response. For example, polio workers were essential to containing the Ebola virus outbreak in 2014. For the Lassa fever response, 271 polio workers are involved in active case search, 235 in contact tracing, and 320 in community sensitization activities across the 18 at-risk states.
“The polio infrastructure was originally designed towards achieving the polio eradication goals,” said Dr Wondimagegnehu Alemu, WHO Country Representative to Nigeria. “Now polio infrastructure has expanded its support to broader disease surveillance strengthening, outbreak response and basic health care services including immunization.”
Other activities carried out by polio workers include data collation and analysis, and case reporting.
“The polio teams on ground in the states were crucial for mounting the initial response to the Lassa fever outbreak, and have continued to be WHO’s frontline technical support to the NCDC, States Ministry of Health and local government area teams,” Dr Emmanuel Musa, WHO Incident Manager for Lassa fever Management Team in Nigeria observed.
A legacy for posterity
Investments by donors and partners have gone far beyond polio eradication. Reflecting the positive impact that polio infrastructure and knowledge has had on other health priorities such as Lassa fever, WHO and other partners are currently supporting the development of a national transition plan. This will ensure that the investments that have brought the world to the brink of eradication are made available to support other national public health efforts, long after polio has been defeated.
“We must carefully consider how we transition many of the polio workers and the polio infrastructure to help with managing other health needs,” Dr Alemu said. “Future funding and partnerships will be a key part of this work.”
For now, experienced polio personnel continue their work to end the Lassa fever outbreak. Thanks to them, and the support of governments, partners and donors, we are ending polio, and are also helping to strengthen other health interventions.
Support for immunization to the Federal Government of Nigeria through the World Health Organization is made possible by funding from the Bill & Melinda Gates Foundation (BMGF), the United Kingdom, the European Union (EU), Gavi, Global Affairs Canada (GAC), the Government of Germany, the Japan International Cooperation Agency (JICA), the Korea Foundation for International Healthcare (KOFIH), the Measles and Rubella Initiative (M&RI) through the United Nations Foundation (UNF), Rotary International, the United States Agency for International Development (USAID), the United States Centers for Disease Control and Prevention (CDC) and the World Bank.
Zulaihatu Abdullahi is well known in her community, particularly to the mothers. As a volunteer community mobilizer in Kaduna state, northern Nigeria, her mission is to ensure that no child contracts polio, or any other preventable childhood disease.
This is difficult, as immunization programmes are sometimes treated with suspicion in her part of Nigeria. As a ‘change agent’, Zulaihatu’s job is to go door to door, counselling parents about the importance of the polio vaccine.
This particular lunchtime, she is visiting an 18 year-old mother living in a compound in a densely-populated, urban district of Kaduna State.
The young mother puts down the pole she is using to pound millet and welcomes Zulaihatu, recognising her royal-blue UNICEF hijab. She sits, and pulls on a hijab for cover as she settles down to breastfeed her baby. She has three other small children at home, a fifth on the way and she is new to the area.
“Before I came here I was rejecting all vaccines,” she says, “but because of this woman, Zulaihatu, I decided to accept. She told me the usefulness and I was convinced to do it.”
Thanks to Zulaihatu’s patience, and her work to build trust with the younger woman through regular visits, four more children are now protected against polio who might otherwise still be at risk. The mother has also been encouraged to seek anti-natal care, and the youngest child has just received his routine immunization shots.
“Sister Zulaihatu was one of the first women I met when we moved here,” the mother recalls. “She came here every day. She told me how she takes care of her own children. What she feeds them. How they all take vaccines. Little by little I started to change my thinking.”
Zulaihatu is trained to make her community aware of important household and parenting practices to keep their children thriving. The list is extensive and includes tips to treat diarrhoea, the importance of basic hygiene and sanitation, how to protect the family from malaria, the benefits of neonatal care and breastfeeding for infants, and the importance of registering their births.
She is one of nearly 20 000 UNICEF-trained community mobilizers, influencers and communication experts spread across 14 northern ‘high risk’ Nigerian states. With the support of donor and partners including the Bill and Melinda Gates Foundation, CDC, Dangote Foundation, European Union, Rotary, GAVI, JICA, the World Bank and the Governments of Canada, Germany, Japan, and others, the mobilizers are a key part of UNICEF’s ongoing support to the Government of Nigeria’s immunization programme.
Despite their achievements, Zulaihatu and other mobilizers know that there is much is still left to be done in their communities. Tomorrow, Zulaihatu will continue her work, going from household to household to keep every child safe.
A bold sign in the camp for internally displaced persons makes it clear where people can come to be vaccinated against yellow fever. WHO/NIGERIA
As he climbs out of his car and walks across to the entrance of Bakassi camp for internally displaced persons in Borno, northern Nigeria, Dr Terna Nomwhange is met by a familiar sight. Standing at the gates, greeting a tired, dusty family laden with possessions, is a team of polio vaccinators. As families arrive at this sea of shelters following a long, hard journey, these people offering polio vaccines are the first sign that they have reached a place of protection.
Not only are families in northern Nigeria facing insecurity, a humanitarian crisis and the threat of polio, but since September they have also been at risk from an outbreak of yellow fever. By early January 2018, a total of 358 suspected cases had been reported in 16 states, with 45 deaths recorded for 2017. In Borno, the ongoing conflict means that the health infrastructure on the ground to respond to the outbreak is limited to local government and the polio eradication infrastructure.
At the camp gates, the polio vaccinators give two drops of vaccine into the mouth of every child; but they also tell the parents where to go to get their yellow fever vaccination. As Dr Terna, who works for the WHO Nigeria polio eradication programme, walks further into the camp, he catches sight of the distinctive blue that signifies the uniform of a polio volunteer community mobilizer. As she emerges from the door of a shelter, he hears her reminding the family within to get their children vaccinated against polio, but also for the whole family to be vaccinated against yellow fever.
With weakened health system in parts of north eastern northern Nigeria, the infrastructure that is already on the ground to stop polio is providing the volunteers needed to support the yellow fever vaccination campaign. More than eight million people are being targeted with yellow fever vaccines in the states of Borno, Zamfara Kwara and Kogi states in 2018.
Vaccinating adults
By providing both polio and yellow fever vaccinations, the polio infrastructure protects everyone – the young children vulnerable to polio, as well as the whole population at risk of yellow fever. WHO/NIGERIA
Regular polio vaccination campaigns reach children under five years of age with polio vaccines, as this age group is the most vulnerable to the virus. But reaching everyone between nine months and 45 years to protect them against yellow fever takes creative thinking. People who would not usually be vaccinated have to be mobilised to come to health clinics where they can receive that one shot of yellow fever vaccine that infers life-long protection.
This is where the polio infrastructure comes in. To prepare for the launch of the yellow fever vaccination campaign that took place at the beginning of February, polio experts supported the preparations by developing detailed microplans, mapping each community so that every individual can be vaccinated. Volunteer community mobilisers, well versed in educating communities about the risks of infection, used their skills to warn populations of the high mortality rates associated with yellow fever.
Surveillance
Volunteer community mobilizers for the polio programme spread awareness of the importance of polio and yellow fever vaccinations. WHO/NIGERIA
The polio surveillance system in Borno is already on high alert to identify any case of polio, even in conflict affected areas. “Surveillance remains everyone’s number one priority,” says Dr Terna. “While the polio infrastructure is doing everything it can to find any trace of polio, it is killing two birds with one stone by keeping an eye out for yellow fever as well. This is a win-win situation to stop both diseases.”
While surveillance focal persons move house to house, they are also raising awareness about the symptoms of yellow fever. When a potential case is found, the polio infrastructure is being used to collect blood samples and transport them to the national laboratory down the reverse cold chain, keeping samples at the correct temperature for testing.
Collaboration
Volunteer community mobilizers for the polio programme spread awareness of the importance of polio and yellow fever vaccinations. WHO/NIGERIA
“What makes this campaign special is not just the fact that the strong polio infrastructure is helping to control other diseases, but also that it underscores what can be achieved with intersectoral collaboration and partnership,” said Dr Wondimagegnehu Alemu, WHO Country Representative to Nigeria. “Without the polio eradication infrastructure, a campaign of this scale would not have been able to take place.”
“Everyone is pulling in one direction – the government, partners and volunteers within communities – to protect any and every vulnerable person against polio and yellow fever,” says Dr Aliyu Shettima, Polio Incident Manager at the Emergency Operations Centre (EOC) in Maiduguri.
Support for immunization to the Federal Government of Nigeria through the World Health Organization is made possible by funding from the Bill & Melinda Gates Foundation (BMGF), Department for International Development (DFID), European Union (EU), Gavi, the Vaccine Alliance, Global Affairs Canada (GAC), Government of Germany through KfW Bank, Japan International Cooperation Agency (JICA), Korea Foundation for International Healthcare (KOFIH), Measles and Rubella Initiative (M&RI) through United Nations Foundation (UNF), Rotary International, United States Agency for International Development (USAID), United States Centers for Disease Control and Prevention (CDC) and World Bank.
The year’s end offers the chance to reflect on the polio programme’s milestones and challenges in 2017, and look ahead to what we can achieve in the coming year. 2017 saw the fewest wild polio cases in history — a total of 17 cases, or a 50% reduction from the year before—with these cases occurring in just two countries: Afghanistan and Pakistan. Yet the need to reach every last child is more important than ever, as demonstrated by surveillance gaps in Nigeria and outbreaks of vaccine-derived polio in Syria and the Democratic Republic of the Congo.
From programme strategies that helped protect progress and overcome obstacles, to commitments from donors and partners, 2017 demonstrated the resolve required to achieve a polio-free future. Accelerating progress in the new year and ending polio for good will require maintaining these political and financial commitments as well as building upon the programme’s efforts to find the virus wherever it exists.
Rooting out the virus
Throughout 2017, developments in disease surveillance – both in humans and in the environment – allowed the programme to better hone in on the virus and identify its remaining hiding places.
These innovations are building robust, sensitive surveillance networks around the world that pick up every trace of the virus and enable the programme to develop targeted immunisation responses before polio has the chance to paralyse children.
The year also came with new challenges, including outbreaks of circulating vaccine-derived polio in Syria and the Democratic Republic of the Congo, where conflict has ravaged the health infrastructure. In these communities, and others where polio still exists, difficult terrain, conflict and highly mobile populations can all stand as hurdles to vaccinating children. Yet the polio programme continues to find new and effective ways of delivering vaccines.
For example, in Afghanistan, a collaboration with a mobile circus is sharing important messages about polio vaccination with hard-to-reach populations, including those living in camps for internally displaced persons. In Pakistan, campaigns based at border crossings and train stations vaccinated children on the move who might otherwise have been missed by traditional methods. And in Syria, dedicated workers are delivering vaccines at transit points and registration centres for internally displaced persons. Thanks to these strategies, more than 255,000 children have been vaccinated in Deir Ez-Zor, 140,000 were reached in Raqqa and the programme continues to work to reach every child.
The mobile circus passed on vital health care and social messages, encouraging full immunization of every child. UNICEF Afghanistan / Ashley Graham
Renewed commitment to end the disease
Complementing these programmatic innovations were political and financial commitments that highlighted polio eradication as a priority for global health leaders. These included:
Next year, country programmes will need to continue working to ramp up surveillance, particularly in Nigeria, and reach children everywhere with vaccines. Cross-border coordination between Pakistan and Afghanistan, which has already had a huge impact in reducing cases, will continue to be critically important to stopping transmission.
At the same time, the global community is beginning to solidify plans for keeping the world polio-free once eradication is achieved. Countries are developing strategies for transitioning the infrastructure and tools that they currently use to fight polio. And the GPEI is working with global stakeholders and partners to develop the Polio Post-Certification Strategy, which will define the activities needed to keep polio from returning after the virus is eradicated.
If the remaining endemic countries continue to do all that they can to stop the virus, and if the global community continues to meet the level of political and financial commitment needed to make and keep children everywhere polio-free, 2018 will bring the world’s best opportunity yet to end the disease.
In Nigeria’s north-eastern Borno state, children displaced by ongoing conflict are being reached with essential immunization and health care services, thanks to a strong network of Volunteer Community Mobilisers established by the polio eradication programme.
Two-year-old Hafsat Khalifa waits patiently in line with her mother, Hadiza. Hadiza is one of many women who’ve brought their young children to receive vital immunization at the local health camp in Maiduguri. Hafsat knows she needs to open her mouth wide when it’s her turn to receive the oral cholera vaccine just like she did when vaccinated with the Oral Polio Vaccine. She displays the confidence of a seasoned pro, although in reality this is the first year she has received any health services, having been born into an area of conflict. Along with these two vaccines, Hafsat will receive other much-needed health care during today’s visit.
Humanitarian crisis
Hafsat is one of many thousands of children affected by the humanitarian crisis in north-eastern Nigeria. The conflict has resulted in a surge in internally displaced persons, with limited access to medical care, leaving millions at risk of life-threatening diseases. Since four cases of wild poliovirus type 1 were detected in Borno in August 2016, an outbreak response for polio has been a top priority. But it has been carried out hand in hand with broader humanitarian efforts to meet the health needs of vulnerable populations.
Benefits beyond polio eradication
UNICEF’s vast network of volunteer community mobilisers have not only played a vital role in ensuring that children like Hafsat receive OPV and other health services every time they are offered, but are leveraging the skill-set they’ve gained from their expanded training to impact child and maternal health far beyond polio.
In addition to receiving the oral cholera vaccine today, Hafsat’s nutrition status will be assessed at the health camp, and children identified as malnourished will be referred for receiving therapeutic food. This important network of polio vaccinators, with years of experience in reaching children with polio vaccines, has made a huge difference in halting the spread of cholera and meningitis outbreaks in Nigeria in 2017. They are also helping create awareness and generate demand for the upcoming campaign against measles.
The reach of this network even extends to protecting children before they are born. Volunteer community mobilisers provide critical antenatal care for pregnant women that can save the lives of mothers and babies alike. And this year, for the first time ever in an emergency humanitarian setting, antimalarial medicines have been delivered on a mass scale alongside the polio vaccine, reaching 1.2 million children in a campaign in August.
For families in Nigeria’s north-east, many who have fled their homes in the face of ongoing violence, this life-line to access essential services is critical to ensuring their children can grow up protected from vaccine-preventable diseases.
The people working to end polio are helping broader humanitarian response efforts in north-eastern Nigeria. With malaria currently claiming more lives than all other diseases put together, a campaign was launched in October to reduce the malaria burden among young children in Borno state by delivering antimalarial medicines. At the same time, community health workers protected children against polio.
“The current campaign marks the first time that antimalarial medicines have been delivered on a mass scale alongside the polio vaccine in an emergency humanitarian setting,” said Dr Pedro Alonso, Director of the Global Malaria Programme, in an interview with WHO on the campaign and the broader humanitarian situation in Borno. “This integrated campaign with WHO’s polio and health emergency teams is an example of unprecedented collaboration to tackle the leading cause of death in a displaced population.”
The humanitarian crisis in north-eastern Nigeria has resulted in a surge in internally displaced persons, with limited access to medical care, leaving millions at risk of life-threatening diseases. In August 2016, four cases of wild poliovirus type 1 were detected in Borno; the outbreak response has been carried out hand in hand with broader humanitarian efforts to meet the health needs of vulnerable populations.
WHO’s well developed network of polio vaccinators, with their years of experience in reaching children with polio vaccines, is making a real difference to the drive against malaria. The polio programme in Nigeria has a vast infrastructure and hundreds of staff on the ground and they are coordinating efforts to make sure that families affected by the crisis have access to other healthcare services.
As a result, the campaigns have reached 1.2 million children with polio vaccines and antimalarial medicines, as shown through a WHO photo story. “I think we will imminently be able to show significant impact,” said Dr Matshidiso Moeti, Regional Director for Africa, reflecting on the encouraging results of the joint campaign.
Africa’s last case? Two-year-old Yafanna Mamma, held by her mother, Yagamallam, in a photo captured by the polio case investigation team. Photo: GPEI
The photo shows a little girl in a blue dress, resting against her mother’s shawl, a tiny green heart hanging from her ear.
It is just over 12 months since two-year-old Yafanna Mamma became Nigeria’s most recently-reported case of wild poliovirus. But this anniversary provides little cause for cheer – last year, Nigeria was about to celebrate two years without any cases, only for four infants to arrive from deep inside conflict-affected territory, in the remote north-eastern state of Borno, paralyzed by polio. Yafanna was the last of them, arriving in the northern Nigerian outpost of Monguno malnourished and sickly.
The discovery of polio in these children underlines the challenges facing the polio eradication programme – and many other health and development initiatives – working in conflict zones. Amidst the ongoing humanitarian crisis in North-Eastern Nigeria, at least 200,000 children are estimated to still live in inaccessible areas, where insecurity is a constant threat. All humanitarian activity, including vaccination campaigns and disease surveillance, is made all the more difficult across these areas, and there is a significant risk that poliovirus continues to hide undetected, spreading among unvaccinated children in the area.
Yafanna’s paralysis was a lesson that when vaccination and disease surveillance efforts pose such a challenge, finding no polio cases does not mean that there is no virus.
Yafanna’s family – father Ali, mother Yagamallam and their two surviving sons – are a living example of the consequences of conflict on the health of families. Their small village, Zanari, is four hours’ walk into inaccessible territory north-east of Monguno, with no health centre and irregular access to vaccination campaigns.
“Since 2014, there is no health facility,” Ali says softly, seated beside his wife in the WHO-UNICEF joint office in Borno’s capital, Maiduguri. “The closest facility is in Monguno town and walking it takes many hours.”
They made that walk, carrying their infant daughter, two weeks after she had fallen sick with a high fever and they soon noticed she could no longer stand. When they arrived in Mongonu a worried doctor quickly referred them to Maiduguri, where they attended a health facility in a camp for internally displaced people.
“At the health facility they asked us to bring stool samples from our daughter, they gave us medicine, and after we went back home. The fever got better, but she stayed paralyzed.”
After two weeks, the military arrived, guarding a medical team which confirmed that little Yafanna, who had never received any doses of oral polio vaccine, had been found by the poliovirus.
“We had heard of this disease,” Ali says, looking down at the table. “But we didn’t know what it could do. Before the insurgency, vaccinators would visit us with a motorcycle. But after the insurgents came the vaccination teams stopped coming.”
The polio eradication programme is working hard in Nigeria to reach every child with the vaccine, and to find the virus wherever it is hiding. Vaccinators are steadily reaching more children, using strategies such as engaging and collaborating with local communities, vaccinating in camps for internally displaced people, and in different locations like markets and transit points. But there is still much work to do.
Little Yafanna never walked again. Three short months later after her paralysis, she contracted another disease – possibly whooping cough – and on 27 December 2016 after three days of coughing and fever, she died.
Ali now has been engaged to talk with the community about the threat of polio, and the importance of vaccination. “I pray that we can honour her life by making her the last polio case in all of Africa. So that her name is remembered. So that her life is remembered.”
A child in Abdulahi Abubakar’s village was paralysed by polio in October 2016. As head of the village he works with religious leaders, local government and health partners to identify cases of polio and encourage vaccination. WHO/J Swan
Surveillance is one of the central pillars of polio eradication. Disease detectives globally are constantly on the alert to find every last virus because without in depth knowledge on where it is, polio cannot be stopped. In northern Nigeria, one of the last remaining places on earth where polio continues to paralyse children, the eradication programme is always on the lookout.
In 2016, Nigeria was taken off the list of polio endemic countries, with two years having passed since the most recent case. Soon after, however, four children paralysed by the virus were found in Borno, a state where insecurity had made some populations inaccessible for several years and where there were gaps in surveillance. A strong outbreak response was launched to stop the virus, despite the challenges.
Strengthening surveillance is an important part of this response. Polio surveillance relies on every case of acute flaccid paralysis (the symptoms of polio) to be found and tested for the presence of the virus, due to the fact that it can be caused by a number of things. To ensure that every case is identified, local healthcare workers, traditional healers, teachers, parents and religious leaders around the world are on the alert for any paralysed child in their communities.
There is still some way to go to improve the Nigeria surveillance system. Work is underway to engage new community informants and to coordinate surveillance efforts with other countries in the Lake Chad region. With an estimated 2.5 million people displaced in the surrounding countries and moving across porous borders, country efforts to identify the virus must work in unison.
The Korea Foundation for International Healthcare
Since 2013, KOFIH, in collaboration with the Community Chest of Korea, has provided US$ 5 million to WHO to fund surveillance in Nigeria as part of its support to disease eradication and emergency relief efforts. With strengthening the surveillance system in Nigeria so central to stopping the virus, the support of the Korea Foundation for International Healthcare (KOFIH) is all the more critical. KOFIH joined with other global health leaders at the Rotary Convention in June who together committed US$ 1.2 billion to the drive to end polio.
“This invaluable support from our partner KOFIH is enabling us to strengthen surveillance in northern Nigeria. Their focus on this challenging area reflects their understanding that in the final throws of an eradication effort, no stone must remain unturned,” said Michel Zaffran, Director of Polio Eradication at WHO.
Young mothers waiting to vaccinate their children receive information on exclusive breastfeeding from a polio-funded Volunteer Community Mobilizer. @ UNICEF/R. Curtis
“Are you watching me?” “Yes, ma’am.”
“Are you seeing me?” “Yes ma’am.”
Along two rows of benches under the awning of the Chikun Primary Health Centre in northern Nigeria’s Kaduna State, about 50 young mothers sit still, their babies swaying on their laps. All eyes are fixed on Lidia, the assured polio social mobilizer who is not delivering polio vaccine, but showing the women how to correctly breastfeed.
Lidia is a grandmother, a one-time community midwife now employed with Nigeria’s polio eradication programme as a UNICEF-supported Volunteer Community Mobilizer (VCM). During the monthly polio vaccination campaigns, she goes house to house with the vaccination team, opening doors through her trusted relationship with the mothers, tackling refusals where they occur and tracking any children missed in the campaigns through her field book containing the names and ages of all children in her area. But it is between campaigns where Lidia’s full worth is realized.
Trust
Helen Jatau, a supervisor in this Local Government Area, supervises 50 VCMs and five first-level supervisors. She is convinced the health care polio frontline workers provide between campaigns provides benefits beyond the surface value – it establishes trust. “When we bring different things to the mothers, it helps the community live better and even accept us more, because we are giving more than just polio vaccines.”
Between polio vaccination campaigns, mobilizers like Lidia track pregnant women and ensure the mothers undertake four Ante-Natal Care visits, including immunization against tetanus. They advise mothers-to-be to give birth at the government health facility, provide them with the first dose of oral polio vaccine, facilitate birth registration and connect them to the routine immunization system. In houses and at monthly community meetings, the mobilizers also provide information on exclusive breastfeeding, hand washing, the benefits of Insecticide Treated Bed Nets, Routine Immunization and the polio vaccination campaign.
Ante-Natal Care
VCM Charity Ogwuche stands before the mothers at the health centre and peels over the pages of a colourful flip book. “Breastmilk builds the soldiers inside your child,” she shouts. “It will save you money. You don’t need to find food for your child to eat. You don’t need to find water: 80% of breastmilk is water. It will protect your child.”
Adiza, a young mother holding her first child, Musa, carries a routine immunization card including messaging on breast feeding and birth registration. “Aminatu talked to me about antenatal care. She asked me to get the tetanus shot, and today she has brought me here to receive routine immunization for my baby. I am really grateful. If she wasn’t here I wouldn’t be here. I wouldn’t know about it. She is the only one who tells me about this.”
Charity is proud of her work. “The women are so familiar with me, it makes me happy. They call me Aunty. I provide most of the health information for them. Really there is no other in our community. They are very young mothers and they need me.”
Birth registration
Aminatu Zubairu, in her trademark blue VCM shawl, displays the birth registration cards she will carry back to mothers in her village. @ UNICEF/R.Curtis
Every Tuesday is birth registration day. Once, hardly a soul turned up to register their newborns, but today, a long line of VCMs are standing clutching handfuls of registration forms, waiting to register the newborns within their catchment area.
Aminatu Zubairu, wrapped in the trademark blue hijab of the VCM, explains how all social mobilizers must come from their own community, and how that familiarity breeds the trust that has enabled her to register hundreds of children in her area. “I go to their houses and ask if they had the birth registration. If they say no I take all the information. Now I will register them and get the certificate of birth and carry it to their house to give back to them. In a month I can do 50 of these. This year there are plenty of newborns.”
Danboyi Juma, the district’s Birth Registration Officer, believes birth registrations have increased by 95% since VCMs assumed responsibility for the service. “They are helping us so much because they go house to house,” he says. “They have increased the number of birth registrations in this area by so much – oh, that’s sure.”
Routine Immunization
Jamila and her baby Arjera, who was vaccinated for the first time, following the persistent efforts of her VCM Rashida Murtala. @ UNICEF/R.Curtis
Despite stifling heat, on this Tuesday, there are more than 50 mothers and several fathers sitting on benches, waiting for their turn to have their babies vaccinated. More than 80% of them carry the cardboard cards given to them by VCMs to remind them their baby is scheduled for routine immunization.
Jamila, a young mother wrapped in a white shawl around her orange head-dress, is bringing her six-month-old baby Arjera to be vaccinated for the first time. Her VCM, Rashida Murtala, badgered her for months before Jamila finally accepted.
“Oh, she refused and refused,” Rashida says. “She’s fed up with me visiting. I went to see her today and finally she followed me. I’m happy to see her here.”
Jamila smiles. “She has been disturbing me every day that I have to take this child to the health centre. I know she’s right, so today I followed her.”
Priscilla Francis, the Routine Immunization provider who vaccinates young Arjera, believes VCMs are key to strong vaccination coverage in Chikun district. “There is much improvement in attendance since the VCMs started. They are well trained. They do a good job of informing mothers to come. If we lost them we would lose our clients – no doubt. When they come we tell them to come back, but no one else is going to their house to bring them.”
Hassana Ibrahim, a Volunteer Ward Supervisor, knows her mobilizers are important. “I have 10 VCMs, five in this ward. Non-compliance used to be a big problem but not now. Now with the routine immunization, the community sees they are providing a package of health care and now people comply with the polio vaccination.”
Naming ceremonies
New mother Naima with newly named Jibrin and her friends and family was happy to welcome her VCM to immunize children at her son’s naming ceremony: “She is my friend.” @ UNICEF/R.Curtis
Following the routine immunization session, the VCMs fan out to attend the naming ceremonies of newborns in their catchment area. Naming ceremonies provide an important opportunity to vaccinate lots of children, as family gathers around to celebrate. On average, they attend 10 naming ceremonies a month. Today we visit Naima, the young mother of a 7-day-old boy, who as per tradition has just been named Jibrin by his grandfather. Naima is surrounded by her sisters, family and village friends, who cook and eat with them, and their 68 children under five. Within minutes, the VCM has walked among them all, vaccinating them as they sit waiting with their mouths open to the sky like little birds.
Naima is happy to see her trusted VCM, and encourages her to vaccinate the children. “I know her well,” she says. “She taught me to go for ante-natal care, to deliver at the hospital and to go for immunization. She is the only health care worker who comes. We are from the same community. She is my friend.”
Just like responding to a polio outbreak, ENDING an outbreak requires in depth data, partnerships and attention to detail. @ WHO
The detection of even a single case of polio anywhere in the world is considered an outbreak. As soon as the polio surveillance system sounds the alert that a virus has been found, an outbreak response springs into action.
But when a virus has so many possible hiding places, how can we be sure it is gone? What enables an outbreak response to be called to an end?
Ending an outbreak: on paper
According to official guidelines, an outbreak is considered to be stopped following a period of 12 months without the detection of any new polioviruses detected from any source, assuming disease surveillance meets certification standards. Once experts are confident that there are no immunity or surveillance gaps that could allow the virus to hide, the World Health Organization (WHO) removes the country from its list of re-infected or endemic countries.
Finding the needle in the haystack
These guidelines set important standards, yet carrying them out in the real world can be complicated. In Nigeria in August 2016, four wild poliovirus type 1 cases were detected. They were caused by a strain that had not been detected since 2012, due to insecurity making disease surveillance difficult in the surrounding area, enabling the virus to move unchecked.
This reminds us that guidelines – while essential – cannot do the job alone. Thorough epidemiological, operational and virological analysis is needed before interruption of poliovirus can truly be verified; and each new outbreak coming to an end must be assessed individually.
Outbreak response assessments
Gathering immunization and surveillance data is crucial to inform outbreak response assessments so that an outbreak can be closed. @ WHO
Every three months in outbreak countries, Outbreak Response Assessments are held by independent experts. They directly observe the implementation of all activities, analyse and verify the data and track how the outbreak is evolving – and whether the response is having an impact. They make recommendations to strengthen the continued outbreak response.
Outbreak Response Assessments provide crucial evidence for programmatic performance, risk management and evolving epidemiology. Without such assessments, we could not verify the continued presence or absence of poliovirus circulation.
Once 12 months have passed with no cases and immunization and surveillance data has been carefully scrutinised through these assessments, the outbreak response assessment committee finally draws its conclusions that the outbreak is over.
International Health Regulations
Information and conclusions from Outbreak Response Assessments are taken into consideration by the Emergency Committee of the International Health Regulations (IHR). Through the IHR, countries work together for global health security, limiting the risk that outbreaks spread across borders. In 2014, polio was declared a public health emergency of international concern under the IHR, leading to temporary recommendations which were put in place for all countries with or at risk of polio to reduce the risk of international spread.
The Emergency Committee on the Spread of Poliovirus meets every three months to review global epidemiology. They draw their own conclusions and classify countries into categories of risk. This helps to stop new outbreaks from taking place and adds an extra pair of eyes to assess when an outbreak has come to an end.
Becoming officially polio-free
Teams of independent experts assess the outbreak response. Only when no case has been found for 12 months can an outbreak be called to a close. @ WHO
The final stamp of approval that a region is polio-free only comes with regional certification. An independent Regional Certification Commission reviews data from all countries in a given region, ensuring that surveillance indicators and vaccination coverage from every single area are of the highest possible levels.
This process takes at least three years. Only when no virus has been detected anywhere in the region for a significant length of time and no doubt is left that the virus is completely gone does a region become certified as polio-free.
Only when no case of polio has been detected anywhere in the world for more than three years will the Global Certification Commission for the Eradication of Poliomyelitis meet to take a decision on whether the virus is truly gone from the world.
No room for complacency
Time, attention to detail and double checking what we know – this is what it takes to end an outbreak.
In the end, the decision to end an outbreak is only as good as the data from each remote village, each sample tested in a laboratory and each vaccination round. This makes knowledge the most powerful tool we have in the fight against polio.
Even once an outbreak has been stopped there is no room for complacency. As long as poliovirus continues to circulate anywhere in the world, countries everywhere remain at risk. As polio moves with people, any population movement to an area of low immunity can lead to a new outbreak.
Until the world has been certified polio-free by the Global Certification Commission, all countries must vaccinate every last child, find every last virus and be prepared for any outbreak.
In early May 2017, polio programme staff from across Nigeria joined efforts to combat a meningitis outbreak in Sokoto, providing support and expertise in outbreak response to help Sokoto State in controlling the outbreak.
Almost 200 WHO polio officers worked with state and national government agencies and other partners to plan and implement a state-wide vaccination campaign aimed at reaching almost 800 000 young people at risk of contracting the disease.
With considerable experience in delivering large-scale vaccination campaigns, polio staff played an important role in the planning, coordination and delivery of the meningitis response. Almost thirty years of fighting polio has equipped GPEI with valuable expertise in outbreak response that can be applied beyond the polio programme.
Working as part of a national support team, they supported the campaign in a number of areas, including the development of a detailed campaign strategy, coordination and logistics, planning, coordination and supervision of trainings, and vaccine management activities.
The broader benefits of the polio programme
This support for meningitis outbreak response is but one example of how the infrastructure and expertise of the Global Polio Eradication Initiative (GPEI) is helping to achieve positive health outcomes beyond polio eradication and can offer significant benefits for broader health efforts. In Nigeria alone, polio staff and infrastructure have contributed to multiple outbreak response and vaccination activities, including the response to Ebola and large-scale measles vaccination campaigns.
Polio-funded workers at country level spend on average 50% of their time supporting non-polio activities, including routine immunization, maternal and child health programmes, humanitarian emergencies and disease outbreak, and sanitation and hygiene programmes.
Skills and infrastructure of the programme in areas like healthcare delivery, disease surveillance and outbreak preparedness and response can be successfully applied to non-polio health priorities and programmes.
Planning for the future
While we remain focused on ending polio for good, GPEI is also beginning to plan for a world after polio – looking at how we can maintain some of this infrastructure, knowledge and expertise once the programme comes to an end. In 16 countries, including Nigeria, with the highest levels of GPEI-funded staff and infrastructure, GPEI partners are supporting national governments and other health partners to plan for the transition some of these critical assets in to existing health systems and initiatives, so they can continue to contribute to positive health outcomes around the world.
A child in west Africa receives polio vaccine. Photo: WHO.
More than 190 000 polio vaccinators in 13 countries across west and central Africa will immunize over 116 million children over the next week, to tackle the last remaining stronghold of polio on the continent.
The synchronized vaccination campaign, one of the largest of its kind ever implemented in Africa, is part of urgent measures to permanently stop polio on the continent. All children under five years of age in the 13 countries – Benin, Cameroon, Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of Congo, Guinea, Liberia, Mali, Mauritania, Niger, Nigeria and Sierra Leone – will be simultaneously immunized in a coordinated effort to raise childhood immunity to polio across the continent. In August 2016, four children were paralysed by the disease in security-compromised areas in Borno state, north-eastern Nigeria, widely considered to be the only place on the continent where the virus maintains its grip.
“Twenty years ago, Nelson Mandela launched the pan-African ‘Kick Polio Out of Africa’ campaign,” said Dr Matshidiso Moeti, WHO Regional Director for Africa. “At that time, every single country on the continent was endemic to polio, and every year, more than 75 000 children were paralysed for life by this terrible disease. Thanks to the dedication of governments, communities, parents and health workers, this disease is now beaten back to this final reservoir.”
Dr Moeti cautioned, however, that progress was fragile, given the epidemic-prone nature of the virus. Although confined to a comparatively small region of the continent, experts warned that the virus could easily spread to under-protected areas of neighbouring countries. That is why regional public health ministers from five Lake Chad Basin countries – Cameroon, Central African Republic, Chad, Niger and Nigeria – declared the outbreak a regional public health emergency and have committed to multiple synchronized immunization campaigns.
UNICEF Regional Director for West and Central Africa, Ms Marie-Pierre Poirier, stated that with the strong commitment of Africa’s leaders, there was confidence that this last remaining polio reservoir could be wiped out, hereby protecting all future generations of African children from the crippling effects of this disease once and for all. “Polio eradication will be an unparalleled victory, which will not only save all future generations of children from the grip of a disease that is entirely preventable – but will show the world what Africa can do when it unites behind a common goal.”
To stop the potentially dangerous spread of the disease as soon as possible, volunteers will deliver bivalent oral polio vaccine (bOPV) to every house across all cities, towns and villages of the 13 countries. To succeed, this army of volunteers and health workers will work up to 12 hours per day, travelling on foot or bicycle, in often stifling humidity and temperatures in excess of 40°C. Each vaccination team will carry the vaccine in special carrier bags, filled with ice packs to ensure the vaccine remains below the required 8°C.
“This extraordinary coordinated response is precisely what is needed to stop this polio outbreak,” said Michael K McGovern, Chair of Rotary’s International PolioPlus Committee . “Every aspect of civil society in these African countries is coming together, every community, every parent and every community leader, to achieve one common goal: to protect their children from life-long paralysis caused by this deadly disease.”
The full engagement of political and community leaders at every level – right down to the district – is considered critical to the success of the campaign. It is only through the full participation of this leadership that all sectors of civil society are mobilized to ensure every child is reached.
Over the years, the Polio Eradication Initiative has been a vehicle for the empowerment of Nigerian women economically and socially. In recent times, this positive development has gained more impact with the timely and direct disbursement of funds for payment of vaccination personnel allowances down to grassroots level.
Over 360 000 vaccinators are engaged to support one round of national polio campaigns, and a further 180 000 for a round of sub-national campaigns. Out of these figures, over 80% are in the northern part of Nigeria where 100% of House-to-House teams are females. In addition, 100% of the supervisors are women. Further profiling of personal for all vaccination teams (including fixed post and transit point teams) indicate that 62% of the vaccinators are females. The findings also showed 88% of them have mobile phones for timely alerts and payments.
Interestingly, most of the female vaccinators are pooling their mobile money so they can have a bigger amount to kick-start their small-scale income generation projects.
“I have been able to successfully establish a business from stipends received from polio campaign and now have a source of income. I acquired a shop, bought machines and fabrics and now, I am the local tailor in my community,” Malama Amina Mohammed, a polio vaccinator team supervisor in Zamfara state mentioned.
There is considerable anecdotal evidence from WHO Nigeria Kano, Katsina and Kaduna state field offices that the huge investments by donors and partners have gone beyond polio eradication to impact positively on the lives of women, thereby enhancing equity.
Happy Gabriel is a student at Kaduna Polytechnic. She became a vaccinator three years ago after gaining admission for her diploma course. Polio programme stipends assisted her to concentrate on her studies and helped greatly to buy books and for her upkeep.
Appreciating the stipends received from SIAs, Happy stated, “I am deeply indebted to the polio immunization programme especially the initiative of Mobile money which eliminates delays we hitherto encountered at payment sites and equally engenders transparency.”
Very soon, Ms Gabriel will obtain her Ordinary National Diploma certificate from an accredited Nigerian institution and be gainfully employed even when polio is finally eradicated.
Asiya Ibrahim in Dala local government area of Kano is a widow. She has been a vaccinator for over six years. She lost her husband shortly before joining the polio programme. The stipends received has been helpful to sustain and keep her house together, including the upbringing of her children such as schooling, feeding and clothing.
With the frequency of the polio campaigns in the north, stipends received after each round cushioned the effect of losing her husband as she is always engaged in some form of activity.
Prior to 2004, operational funds to support SIAs in Nigeria were deposited by partners in a central dedicated account managed by the central government agency responsible for disbursement of the funds to vaccination teams. This mechanism faced a number of challenges including under-payment or non-payment of end-beneficiaries, delays in payment and retirement and inadequate documentation.
WHO conducted a risk assessment in 2013 and then established the Direct Disbursement Mechanism; an innovation that is considered a best practice and emulated by wide range of stakeholders.
With the innovation, the polio programme has helped to build up lives of vulnerable and economically disadvantaged personnel, especially those of women especially in poverty-stricken villages of northern Nigeria. The allowances after each round of SIAs have made them responsible to their immediate families and environment.
Polio interruption impossible without women
While monitoring the February 2017 round of SIAs in Kano, Dr Wondi Alemu, the WHO Country Representative, underscored the important role of female vaccinators who “are doing a marvelous job of fighting polio by negotiating and engaging with parents even when on transit. Without these women, the fight against polio will not be completed in Nigeria. The mothers trust them as they use techniques, including gestures and understandable language to convey much more meaning that easily persuades erstwhile resistant caregivers”.
Dr Alemu strongly feels that one lesson learnt from PEI is that the success of any public health intervention in Nigeria, especially in the north, hinge on the active participation of women who have empathy and patience to deal with diverse human emotions.
Additionally, through numerous training schedules and other activities organized by WHO and other GPEI partners preceding SIAs round, women’s skills have been empowered. Such skills as interpersonal communications skills, including negotiations have immensely contributed to resolving non-compliance to the oral polio vaccine among difficult to convince populations in northern Nigeria.
Nigerian Minister of Health (left) and EU Ambassador signing the documents for the €70 million grant
At an event in Abuja on 16 February 2017, the Government of Nigeria and the European Union signed a historic partnership to support health systems and polio eradication efforts in the country. Attended by key ministries and partners such as WHO and UNICEF, a €70 million grant agreement was signed targeted at improving maternal, newborn and child health, strengthening Nigeria’s health system and supporting ongoing efforts to eradicate polio.
The project is the first phase of support from the European Union to the Nigerian health sector under the 11th European Development Fund, and will be jointly implemented by United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO) in partnership with the Federal Government of Nigeria and key target states in the country.
Fifty million euro of the grant aims to ensure that by 2020, Adamawa, Bauchi and Kebbi states of Nigeria have functional primary health care centers, providing round-the-clock services to three million children under the age of five years as well as to almost a million pregnant women and lactating mothers.
Twenty million euro, to be dispersed by WHO, will go specifically towards health systems strengthening to achieve universal health coverage and support the push to eradicate polio from Nigeria for good. The grant comes at a critical time for polio eradication in Nigeria, with emergency efforts underway to stop the virus in the last remaining polio reservoir on the African continent.
Michel Arrion, the EU Ambassador to Nigeria and ECOWAS, said at the event, “The European Union is working together with the Nigerian authorities to address developmental challenges in key priority areas under its 11th European Development Fund. This project will help to improve access to effective health and nutrition in the prioritized states and support the final push to eradicate polio in Nigeria”.
The EU has been major supporter of polio eradication efforts worldwide and in particular Nigeria, providing €45 million to the country between 2011 and 2017. Additionally, the EU has provided significant emergency funding to help successfully stop past outbreaks in the Horn of Africa and the Middle East, and supported the eradication effort in other parts of the world.
Thanking the EU for on-going commitment, Dr Wondimagegnehu Alemu, WHO Country Representative, said, “Our partnership with the EU will enable the organization to continue providing the necessary technical support to the government of Nigeria towards strengthening health systems and enhancing timely interventions during supplemental immunization activities, including reaching children in areas with insecurity in the northeast.”
Polio eradication efforts have always played an important role in health systems strengthening. The polio network routinely conducts surveillance for other diseases of public health importance, including measles, yellow fever, neonatal tetanus and avian influenza. With local knowledge of communities, health systems and government structures, the polio network’s technical capacity in disease surveillance and planning of large-scale operations often helps sustain international and national relief efforts. At the country level, polio staff spend, on average, 50% of their time working on broader public health efforts, over and beyond polio eradication, providing a critical contribution to strengthening of health systems.
A US$ 33.3 million grant from the Government of Japan in humanitarian emergency funding to UNICEF was announced this week and will help to protect millions of children from polio in Nigeria and the Lake Chad region.
In response to the urgent need to rapidly raise immunity to polio virus in the region, Japan has generously provided exceptional funding from their supplementary budget envelope to purchase polio vaccines, conduct house-to-house polio campaigns and support communication efforts to mobilize communities for vaccination in Nigeria, Chad, Niger, Cameroon and the Central African Republic.
The detection of wild poliovirus in north-eastern Nigeria occurred in August 2016 following the large-scale movement of families affected by conflict in Borno State out of areas inaccessible to health services. National Governments, in collaboration with the Global Polio Eradication Initiative (GPEI), comprising the World Health Organization, UNICEF, Rotary International, CDC and the Bill & Melinda Gates Foundation (BMGF), have implemented emergency vaccination campaigns throughout the region to rapidly raise childhood immunity to the polio virus and guard against further spread.
UNICEF Director of Polio Eradication Mr Reza Hossaini said the Japanese funding was gratefully received and filled an urgent need. “This additional funding is very timely to support the ongoing polio vaccination campaigns and give Africa the very real opportunity to be completely polio-free,” Mr Hossaini said. “These campaigns aim to not only stop transmission of polio in north-eastern Nigeria but protect its neighbours against the spread of the virus through provision of vaccines and targeted social mobilization activities.”
Japan remains one of the champion donors to the GPEI and the Global Health agenda in general, with contributions to polio eradication through UNICEF since 2002 totalling more than US$ 333 million. This funding – and the leadership provided by both the Tokyo International Conference on African Development (TICAD) process and the Japan International Cooperation Agency (JICA)’s innovative soft loan in partnership with BMGF in Nigeria and Pakistan for polio eradication – has proven instrumental in the historic reduction of wild poliovirus transmission globally.
In 2016, wild poliovirus transmission was limited to just 37 cases globally in the three remaining polio-endemic countries – Nigeria, Pakistan and Afghanistan. This year, to date, only two cases have been recorded worldwide, in Afghanistan. However, while the opportunity to finally eradicate polio is real, the risk remains: as long as one child is infected, every child remains at risk. It is critical that all countries continue to maintain high immunity to polio until the virus is eradicated, once and for all.
A health worker prepares to administer a vaccine in northern Nigeria. WHO/L.Dore
A mass vaccination campaign to protect more than 4 million children from a measles outbreak in conflict-affected states in north-eastern Nigeria started on 13 January. The polio eradication infrastructure has been on hand to help with this feat of logistics. GPEI partners WHO, UNICEF and US Centres for Disease Control have been working with nongovernmental organizations to support the campaign in a range of areas including data management, training, social mobilization, monitoring and evaluation, supportive supervision and waste management.
“Nigeria’s well-established polio vaccination programme provides a strong underpinning for the campaign,” says Dr Wondimagegnehu Alemu, WHO Representative in Nigeria. “Population data from the polio programme has been essential to guide planning for the measles campaign. We are also able to make use of staff that have vast experience in providing health services in very difficult and risky areas.”
One third of more than 700 health facilities in Borno State, north-eastern Nigeria, have been completely destroyed, according to a report released in December by WHO. Of those facilities remaining, one third are not functioning at all. This is leaving the health of communities vulnerable.
WHO has a strong presence in the community in these areas thanks to a well-established polio programme which includes teams of health workers trained to work in areas of high insecurity and reach communities that no other partner can reach.
With levels of malnutrition as high as 20% in some populations in Borno State, children are particularly vulnerable to diseases like measles, malaria, respiratory infections and diarrhoea.
Planning for the future
This measles campaign in northern Nigeria is by no means the only example of polio funded functions and infrastructure contributing to other critical functions. On average, polio-funded staff spend more than 50% of their time on non-polio activities, such as routine immunization, measles campaigns, maternal and child health initiatives, humanitarian emergencies and disease outbreak, sanitation and hygiene programmes and strengthening health systems. In Nigeria in 2015, the Emergency Operations Centres set up to tackle polio were repurposed instantly in response to the spread of Ebola to the country, which enabled the outbreak to be ended almost as soon as it began.
Polio is closer to eradication than it has ever been; and while we keep all efforts on rooting out the virus in its final hiding places, the Global Polio Eradication Initiative is also beginning to plan for the future. The 16 priority countries, including Nigeria, where 95% of the programmes assets are based are planning now so that some polio funded functions and infrastructure can continue to contribute to other critical health and development goals, as polio funding gradually decreases
Read more about the measles vaccination campaign in Nigeria.
In August 2016, hundreds of thousands of people fled their homes in Borno State, north-eastern Nigeria, where they had been living in areas under the control of the armed group Boko Haram. These areas had been inaccessible to any health programme, including polio vaccinators.
When health workers finally reached these families, they found thousands of severely malnourished children in need of treatment for a range of health conditions. They also found four children in three different locations within Borno paralyzed by polio. The virus had been spreading silently in these areas for the past two years, beyond the reach of the polio eradication programme.
The detection of polio in Nigeria was a serious setback for the polio eradication programme. With no cases detected in Nigeria or any other African country for two years, there was hope that Africa was polio-free.
The outbreak response was swift and comprehensive, with the Governments of Borno and Nigeria, the World Health Organization and UNICEF conducting an immediate emergency vaccination response.
From August, health authorities conducted five large-scale supplementary vaccination campaigns targeting every accessible child under five years of age in Borno State. Campaigns were also aimed at children in the bordering states of Nigeria, as well as the Lake Chad region of Niger, Chad, Cameroon and the Central African Republic in synchronized activities to rapidly raise childhood immunity to the poliovirus and protect against inter-state and international spread. Approximately 11 million children are being targeted across the region.
Multiple strategies were employed to reach as many children as possible. Additional health workers were hired and trained and detailed plans for each settlement and internally displaced persons camp were comprehensively reviewed to ensure all children were registered for immunization. Targeted media campaigns drew awareness to the upcoming vaccination campaigns. Health camps offered polio vaccination in addition to basic health care packages.
To accelerate community demand for vaccination, the Volunteer Community Mobilization Network was quickly scaled up to reach all highest-risk communities. These women, in their distinctive blue hijabs, move from house-to-house and through the internally displaced persons camps to ensure parents know about the risk of polio and the importance of full immunization for their children. Working for just a couple of dollars a day, they also connect pregnant women to available health services and encourage safe delivery practices, as well as identifying children with severe acute malnutrition and linking them to treatment facilities.
Health camps have been set up in areas with a high number of internally displaced persons to offer much-needed health services than polio vaccines alone. These include de-worming tablets, zinc, oral rehydration salts for children with diarrhea as well as other routine vaccinations for children who may never have had contact with a health system. Polio survivors help to educate parents at these camps to the dangers of the current outbreak and the fact that there is no cure for polio, but that it can be prevented through vaccination.
To access the hardest-to-reach populations in newly-accessible areas, the Government of Nigeria with support from the United Nations is using helicopters to deliver vaccines and other health services. UNICEF has procured and delivered more than 150 million doses of oral polio vaccine to this outbreak response. The work remains dangerous, with ongoing attacks and active fighting in some areas.
After having access to so little for so long, the demand for services has been overwhelming from affected communities. The provision of soap and other basic ‘pluses’ has helped to meet some of these needs, and encouraged mothers to bring their children out for vaccination.
With so much at stake, strong monitoring and supervision has been key to ensuring as many children can be reached as possible. Wide-scale vaccination campaigns offering polio vaccination and other services will continue throughout the first quarter of 2017 in an effort to ensure this outbreak is stopped and the world can finally achieve a polio-free Africa, once and for all.
A child in northern Nigeria receives a dose of the oral polio vaccine. Vaccination teams are going to great lengths to protect every last child against polio. UNICEF/T.Moran
Experts from across the Global Polio Eradication Initiative (GPEI) partnership convened an emergency meeting in Abuja, Nigeria, from 3 – 5 November. Led by senior epidemiologists from the governments of Nigeria and neighbouring countries, the group examined a detailed review of the current impact of the outbreak response, and identified area-specific challenges and prioritized operational plans accordingly.
The detection of new wild poliovirus type 1 (WPV1) cases in Borno, Nigeria, in August – the first detected on the African continent in more than two years – has prompted an unprecedented response. The outbreak was immediately declared by both the Government of Nigeria and governments of surrounding countries to be national and regional public health emergency. This opened the way for a regional outbreak response, mobilizing emergency resources from across the public and civil society sectors.
Thousands of health workers across the region have been mobilized and trained, and in Borno alone more than 1.7 million children have been vaccinated. But many more continue to be un- or under-immunized, either due to operational deficits in outbreak response implementation, hampered access due to insecurity or large-scale population movements within countries.
Unless these missed children are rapidly reached, the risk remains that the current outbreak could spread further, including internationally, and cause more preventable, incurable paralysis.
Access and reaching populations everywhere
Insecurity, geographical challenges and difficulties with communication in some of the hardest to reach areas are providing barriers to reaching all children. Internally displaced persons (IDPs), refugees and nomads are particularly vulnerable groups, with insecurity blocking transit routes and the ability to accurately predict population size ahead of vaccination campaigns reduced. Due to population displacement, detailed micro-plans are frequently disrupted.
Children across northern Nigeria and other countries in the Lake Chad region must be protected rapidly against polio to end the outbreak. UNICEF/T.Moran
Cross-border coordination, embedding the response within the broader humanitarian emergency context, and innovating rapidly to adapt strategies to local challenges is what has stopped similar outbreaks with similar challenges elsewhere in the world.
Yet despite these challenges, the GPEI can draw on a vast array of experience from running outbreak responses in similar settings, most recently in the Middle East, Central Africa and the Horn of Africa from 2013-2015. These existing, proven strategies are rapidly adapted to the evolving environment. Permanent vaccination teams are now in place, as and when an area becomes accessible, to rapidly implement ‘mini’ vaccination campaigns in between larger-planned activities. Such teams are also critical to reach populations as they leave inaccessible areas. Children in both formal and informal IDP camps are a particular focus for the delivery of the polio vaccine alongside other humanitarian and basic health needs.
Assuming that many children living in conflict-affected areas will not have been vaccinated for several years, the target age group has been raised to protect children over 5 years of age.
The Volunteer Communication Network of vaccination advocates within communities has been expanded to cover Internally Displaced Populations living in camps and host populations, while Koranic School teachers have been engaged to address non-compliance and the mobilization of women and youth to ensure local protection for vaccination teams.
Volunteer community mobilizers wearing distinctive blue hijabs are working in IDP camps and host communities to identify unvaccinated children, pregnant women and those with severe acute malnutrition. UNICEF/T.Moran
Coordinating across borders
While cases of polio have only been found in Borno, extensive population movement, insecurity and previous cross border population movements require the outbreak response to cover the entire Lake Chad region. Cameroon, the Central African Republic (CAR), Chad, Nigeria and Niger are working together to track population movements and addressing the challenges inherent in accessing some hard-to-reach areas in each country, including sourcing communication equipment to operate where there is a lack of telecommunication network, closed borders in some places and language barriers. Efforts are being intensified to map out the seasonal movement of nomads, identifying resting places and water points with the support of nomadic community leaders in order to improve micro-planning to inform the response. In Chad, vaccination campaigns are providing livestock vaccines alongside polio vaccines to children in order to increase uptake in nomadic communities.
It is not insecurity alone that leads to hampered access. Sometimes it is simply a more natural phenomenon: the rains! The rainy season in the region typically runs from June to mid-October. Some areas are completely cut off from roads and other transport networks as a result of the associated flooding. With the rainy season now over, many areas and populations will be able to be reached with polio vaccine and other urgent health services.
Stopping outbreaks in such challenges settings is possible
There is no doubt that running an outbreak response with such challenges is far more complex, dangerous, costly and slower than under normal circumstances. However, what is equally clear is that the plans being intensified and implemented across the region are having an impact, and will continue to have an impact. Cross-border coordination, embedding the response within the broader humanitarian emergency context, and innovating rapidly to adapt strategies to local challenges is what has stopped similar outbreaks with similar challenges elsewhere in the world.
The groundwork set by this first phase of the outbreak response has set for reaching previously missed children in late 2016 and throughout 2017.
With continued leadership of political, health and community leaders at the local, national and regional levels alongside the international development community, this outbreak will be stopped and children across Africa protected against polio.
To find out more, the Global Polio Eradication Initiative (GPEI) spoke to Rob Holden, WHO Overall Incident Manager and Pascal Mkanda, regional polio coordinator for WHO’s Regional Office for Africa, who talk about working as ‘one WHO’, combining resources, playing off comparative advantages, a unique ability to work in areas not accessible by other agencies or partners, and ensuring Africa remains on track for polio-free certification.
GPEI: WHO and its partners are engaged in a polio outbreak response in north-eastern Nigeria, but it is being conducted within a broader humanitarian emergence response in the region. Why?
Rob Holden: I think the very first thing to say is that nothing is going to detract from Africa’s goal of becoming polio-free. All countries across the continent have worked incredibly hard to bring Africa to the brink of being polio-free, and this outbreak will be stopped rapidly and the region will be rapidly certified. The most effective way to achieve this, in the current emergency context, is to actually conduct the outbreak response within the broader humanitarian response. And there are many reasons for this. Firstly, it makes sense from an operational point of view. The GPEI has a vast infrastructure and staff on the ground. So have we. It makes sense to coordinate and align our efforts. But most importantly is the humanitarian aspect of the response. We cannot just deliver polio vaccine to populations who have not had access to basic healthcare or even food in months. We have to ensure that the populations receive what they actually need. Yes, there is a polio outbreak and they need vaccines to protect them from this virus. But over and beyond that, they need much more at the moment.
Pascal Mkanda: Rob is right. If you think about the current situation on the ground: the main areas affected by the humanitarian emergency are Borno, Yobe, Adamawa and Gombe states. Approximately 50% of the population is affected by this emergency. There are almost two million internally displaced persons, along with approximately 155,000 refugees in Chad, Cameroon and Niger. Access to health services has been drastically compromised, with half of the population not having access to any basic health services. This is significantly increasing the threat of disease outbreaks, and is resulting in high levels of morbidity due to common ailments such as malaria, acute respiratory infections, diarrhoea, and others. Acute malnutrition is increasing, leading to further medical complications and exacerbating severity of common ailments. In total, seven million people are in urgent need of humanitarian assistance. We cannot deliver aid in isolated silos. We have to try to deliver the full package of what the populations and communities need most urgently. It makes sense operationally, it makes sense politically, it makes sense from a public health point of view and from a cost-effectiveness point of view. But most importantly, it makes sense from a humanitarian point of view. It’s really the only way to operate.
Rob Holden: Incidentally, this is also how the polio outbreak responses were successfully run recently in the Middle East and the Horn of Africa.
GPEI: How does it concretely work on the ground?
Rob Holden: It’s very challenging. One thing is to get medical supplies of aid on the ground. The other is to ensure that it actually reaches those groups of people that it needs to. And in an area affected by lack of infrastructure, large-scale population movements or inaccessibility due to insecurity, it makes it very challenging regardless of whether you want to deliver polio vaccine or an oral rehydration table. But at the same time, since our challenges are the same, so are our solutions. So we tap into one another’s networks and make sure we work hand in hand and as we reach populations we reach them with a more comprehensive package of aid.
Pascal Mkanda: It means that in the first instance within WHO, we – meaning the emergencies and polio teams – work hand in hand on a day-to-day basis. At all levels of the organization, whether at global, regional, national, state-level or at Local Government Area level. Who has what staff and capacity on the ground, and where? What do they need? What can one group or the other provide rapidly? What is the latest information or data that your teams can share, to help maximise the impact of the response? This day to day interaction is critical for planning and operational purposes. We are operating as ‘one WHO’.
Rob Holden: And this same internal modus operandi is then extended to other partners. Of course we work with the government on the ground. But as importantly, we work in this way with other UN agencies and NGOs on the ground, to ensure we contribute in a strategic and targeted way, complementing each other’s works rather than duplicating it. Much has been learned since the 2004 Tsunami in Southeast Asia, in terms of coordinating complex emergency humanitarian response among the humanitarian sector. Everyone recognizes that everyone has the same challenges, and our response must be the same. That is the aim, though for sure in such complex settings as north-eastern Nigeria it is very difficult. But the fact is: we have a network of more than 2,000 staff and volunteers on the ground. They have vast know-how, including of the local environment. As a result, we are able to operate in locations where at the moment no other agency or partner is able to operate. This puts us in a hugely advantageous position, and the overall response must capitalise on that.
GPEI: What exactly is WHO’s role then in this coordinated humanitarian response?
Rob Holden: WHO’s remit and technical expertise is of course to support the Government and its leadership in strengthening the provision of basic health services. The provision of evidence-based technical guidance is a key strength of our organization. That is one of our main areas of focus, in support of the Government at all levels, to address the primary healthcare crisis that has emerged, and try to close this gap in service provision. As such, we work closely with the State Ministry of Health in Borno, to coordinate the health sector response, with particular focus on reaching areas and populations most acutely in need. This includes delivery of basic health services such as vaccinations, enhancing surveillance for epidemic-prone diseases, providing life-saving interventions to manage common ailments among children, adult and the elderly, and improving maternal and child health services at the community and facility level including mentoring of health workers. We then are in a constant state of evaluating the impact of the interventions, which allows us to put in place corrective measures based on these analyses.
Pascal Mkanda: Populations in complex emergencies are more vulnerable to diseases such as polio. That is why a strong focus is placed on putting in place robust disease surveillance and investigation mechanisms, to rapidly identify any major outbreaks of any disease and enable a rapid and robust response. In that sense, the polio outbreak will be a real proof-point for how the broader response is working. It was identified and is now being responded to. An emergency within an emergency, as it were. Progress and success addressing it will tell us a lot about how the overall humanitarian response is being implemented. And of course as WHO, it is about maximising our comparative advantage within the broader response. We help deliver health interventions. At the same time, organizations such as the World Food Programme for example help deliver food. The polio team provides of course the polio vaccine. But the point is: all these different programmes and organizations all have their own staff and infrastructure on the ground. It is all in our interest to deliver our ‘products’ as it were to the populations who need them the most. So by working together, we can increase our reach and make the biggest impact. That’s the overall aim and it’s really the only way to work.
Much attention has rightly been given to the recent detection of wild poliovirus type 1 (WPV1) cases in Nigeria, the first reported from the African continent in more than two years. The announcement of these cases came on the eve of Africa’s ‘two year’ anniversary without polio. But even without detection of these cases, the risk of an ongoing circulating vaccine-derived poliovirus strain type 2 (cVDPV2) had also remained, in Guinea.
Guinea has been affected by a cVDPV2 outbreak, centred around the country’s Kankan region, since 2014. While no new cases have been reported since December last year, remaining subnational surveillance gaps in the region mean that undetected circulation cannot be ruled out.
Guinea has made strong improvements both to its population vaccination/immunity levels – which had been decimated as a result of the Ebola crisis – and surveillance sensitivity over the past year. An official outbreak response assessment found profound and significant improvements across the country. Despite these improvements, however, gaps both in vaccination coverage and surveillance remain which must be filled, before it can be definitively concluded that the outbreak has been stopped.
Worryingly, as many as 20% of children in Kankan remain underimmunized and therefore vulnerable to diseases such as polio. Of additional concern is that neighbouring countries, in particular those which had also been affected by Ebola, also have significant immunity gaps in key areas. In Liberia for example, in some areas as many as half the children are not fully protected against polio.
This should be cause for concern and a need for urgent action, particularly given the risk of undetected circulation of the cVDPV2 in the region, and now with the detection of WPV1 in Nigeria. Historically, WPV1 from northern Nigeria has repeatedly spread to re-infect countries across west Africa.
The risk of persistent subnational gaps – both in surveillance and population immunity – was highlighted and underscored at the recent Africa Regional Certification Commission meeting, not just in west Africa, but indeed across west, central and the Horn of Africa. Despite tremendous progress achieved across the African continent towards polio eradication, detection of recent viruses and persistent surveillance and immunity gaps are a stark reminder that more must be done to secure a lasting polio-free Africa once and for all.
Nigeria has been experiencing insurgency in the north-eastern part of the country since 2009 which led the Nigerian President to declare the state of emergency in the 3 worst affected states of Borno, Yobe and Adamawa states in May 2014.
The Global Polio Eradication Initiative (GPEI) aims to deliver polio vaccine alongside broader life-saving health interventions to some of the most marginalized populations globally in order to fulfil the goals of the Endgame plan. As part of the humanitarian response to the current crisis in Nigeria, a holistic approach to tackling polio underpins the current outbreak response efforts.
A deteriorating humanitarian situation
Against a backdrop of long-term crisis, the humanitarian situation in northern Nigeria has worsened substantially in recent weeks. Over seven million people are in urgent need of humanitarian assistance across the country, with limited access to basic health and other essential services, with the main areas impacted by the crisis situated in the north-east. Access to health services has been drastically compromised, with half of the population not having access to any basic health services. As a result on-going public health risks are very high, with low baseline vaccination coverage rates, populations housed in overcrowded and unsanitary camps and severe food insecurity. The crisis also has broader regional implications, with approximately 155 000 refugees in Chad, Cameroon and Niger.
Challenges to polio eradication
This difficult situation was made more complicated by the detection in August in Borno of two new cases of polio – the first cases detected in Africa since 2014. As many as 600,000 children across north eastern Nigeria remain inaccessible to polio vaccinators, presenting a very real obstacle to polio eradication efforts. Concrete strategies are in place to tackle such obstacles, including through close collaboration with key community stakeholders. Similar approaches have been used by the GPEI in other parts of the world beset by complex humanitarian emergencies or insecurity. Most recently in the Middle East, the polio outbreak response was conducted within the broader humanitarian response effort, to ensure that as communities are reached, they are not just reached with polio vaccine but with a host of other lifesaving health interventions.
An effective outbreak response
Following the recent cases of polio in Nigeria, a major vaccination campaign in Nigeria and the surrounding region has been launched in collaboration with the Ministry of Health and UNICEF, with subsequent rounds to follow. Vaccination efforts form part of the broader response to the current humanitarian crisis in Borno and the surrounding states, and across the Lake Chad basin countries. The focus is on coordinating the delivery of basic health services including vaccinations, enhancing surveillance for epidemic-prone diseases, providing life-saving interventions to manage common ailments among children, adult and the elderly, improving maternal and child health services at the community and facility level including mentoring of health workers, conducting ongoing evaluations of the evolving situation, and improving readiness response for any new disease outbreaks. The GPEI is committed to integrating within a broader humanitarian framework in order to secure a polio-free world.
Following the recent detection of wild poliovirus in Nigeria, Ministers of Health from Cameroon, Central African Republic, Chad, Niger and Nigeria have declared the polio outbreak in Nigeria as a public health emergency for countries of the Lake Chad basin. The declaration, coming out of the 66th session of the World Health Organization Regional Committee for the African Region, demonstrates commitment from governments across the region to bolster momentum in the fight against the virus.
A regional response to a regional risk
The declaration requests that Nigeria and all countries of the Lake Chad Basin, as a matter of the utmost urgency, fully implement coordinated outbreak responses in order to quickly interrupt this outbreak before the end of 2016 and prevent international spread. It calls on all Member States of countries of the Lake Chad Basin to extend all possible support, including political advocacy and engagement at all levels, for successful coordination and implementation of synchronized polio vaccination activities across the countries of the Lake Chad sub-region. The declaration builds on the sustained commitment of member states across the region in the path towards polio eradication, highlighted at the African Union summit in June 2015 where African heads of state gathered to declare polio eradication a “historical legacy for future generations”.
Immediate action, challenging terrain
An immediate response was mounted by the Nigerian government following the outbreak by quickly declaring it as a public health emergency and mobilizing the needed resources, with a large-scale vaccination campaign implemented and further rounds planned across the Lake Chad sub-region.
While challenging terrain lies ahead in beating the poliovirus for good, in Nigeria, and in Africa – not least because of the grave humanitarian situation in many of the countries around Lake Chad – the declaration of a regional emergency provides an important foundation for action, including the mobilization of necessary financial, political and technical support from partners of the Global Polio Eradication Initiative and governments across the region.
Geneva 11 August 2016 – After more than two years without polio in Nigeria, the Government reported today, that two children have been paralyzed by the disease in the northern Borno state.
As an immediate priority, the Government of Nigeria is collaborating with the World Health Organization (WHO) and other partners of the Global Polio Eradication Initiative to respond urgently and prevent more children from being paralyzed. These steps include conducting large-scale immunization campaigns and strengthening surveillance systems that help catch the virus early. These activities are also being strengthened in neighbouring countries. In response to confirmation of these cases, the Government of Nigeria declared this outbreak as a national public health emergency.
Genetic sequencing of the viruses suggests that the new cases are most closely linked to a wild poliovirus strain last detected in Borno in 2011. Low-level transmission of the poliovirus is not unexpected, particularly in areas where it is difficult to reach children with the vaccine. Subnational surveillance gaps persist in some areas of Borno, as well as in areas of neighbouring countries.
“We are confident that with a swift response and strong collaboration with the Nigerian Government, we can soon rid the country of polio once and for all. This is an important reminder that the world cannot afford to be complacent as we are on the brink of polio eradication – we will only be done when the entire world has been certified polio-free,” said Mr Michel Zaffran, Director of polio eradication at WHO Headquarters.
As recently as 2012, Nigeria accounted for more than half of all polio cases worldwide, but the country has made significant strides, recently marking 2 years without a case on 24 July 2016. This progress has been the result of a concerted effort by all levels of government, civil society, religious leaders and tens of thousands of dedicated health workers. Recent steps including increased community involvement and the establishment of Emergency Operations Centers at the national and state level have been pivotal to Nigeria’s capacity to respond to outbreaks.
A child’s finger is marked after being vaccinated. Bodinga, Nigeria photo:Christine McNab
Independent polio campaign monitoring is carried out to assess the quality and impact of supplementary immunization activities. It is critical to guiding any necessary mid-course corrections if gaps or problems are found.
The basic elements of monitoring include recording: the number and source of independent monitors, the number of children monitored, the percentage of children whose fingers are marked to prove they were vaccinated (both in house-to-house monitoring and out-of-house) and the proportion of districts monitored.
Real-time, independent monitoring data answers the question, “How many children did we reach with vaccine?” It allows rapid changes to be made to cover missing children and stop polio transmission more quickly.
The results of the independent monitoring are made available internationally within 15 days of each immunization round.
Reports by country are available through the menu on the left.






































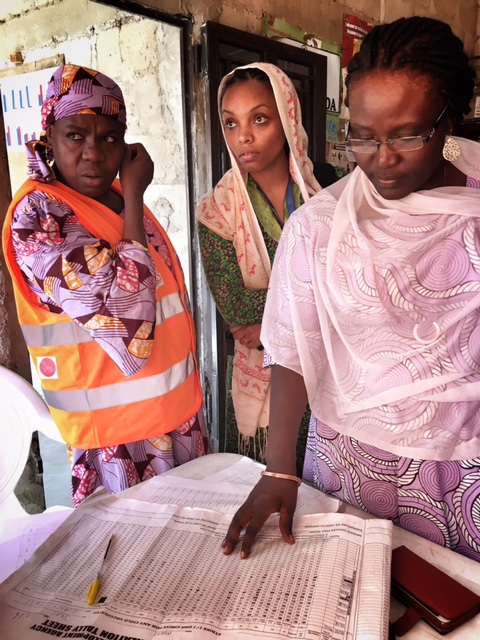




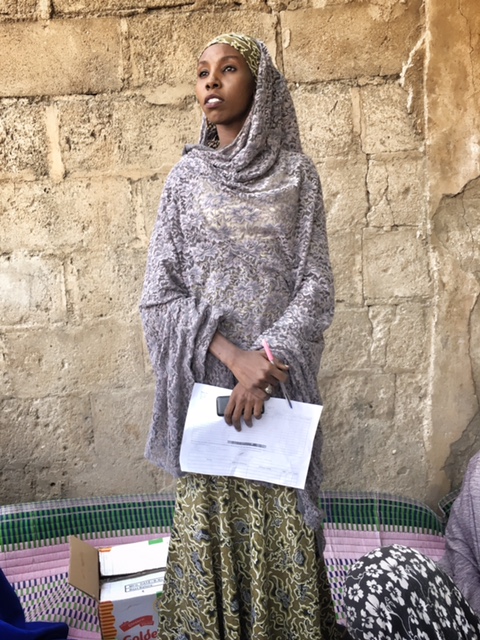




 Much attention has rightly been given to the recent detection of wild poliovirus type 1 (WPV1) cases in Nigeria, the first reported from the African continent in more than two years. The announcement of these cases came on the eve of Africa’s ‘two year’ anniversary without polio. But even without detection of these cases, the risk of an ongoing circulating vaccine-derived poliovirus strain type 2 (cVDPV2) had also remained, in Guinea.
Much attention has rightly been given to the recent detection of wild poliovirus type 1 (WPV1) cases in Nigeria, the first reported from the African continent in more than two years. The announcement of these cases came on the eve of Africa’s ‘two year’ anniversary without polio. But even without detection of these cases, the risk of an ongoing circulating vaccine-derived poliovirus strain type 2 (cVDPV2) had also remained, in Guinea.


