Front-line health workers and volunteers represent the backbone of the global polio eradication effort. As they work tirelessly to reach and vaccinate every last child against polio – often in remote, hard-to-reach or even dangerous areas – they are not only protecting children from the poliovirus, but also paving the way for other health programmes to reach the world’s most vulnerable children.
The Every Last Child project is a collection of over 30 stories and profiles from India, Pakistan and Afghanistan about the collective efforts of front-line health workers, governments and global health partners to protect children from the poliovirus in some of the world’s most challenging environments. These multimedia pieces illustrate the complexity and scale of polio eradication efforts in each of these key countries through in-depth narratives, compelling profiles and interactive visuals.
To end polio, the global polio programme must reach every last child and take bold steps to take the world across the finish line once and for all. Visit the Every Last Child project page to learn more about the history of these remarkable efforts, as well as stories of heroic front-line workers.
In September
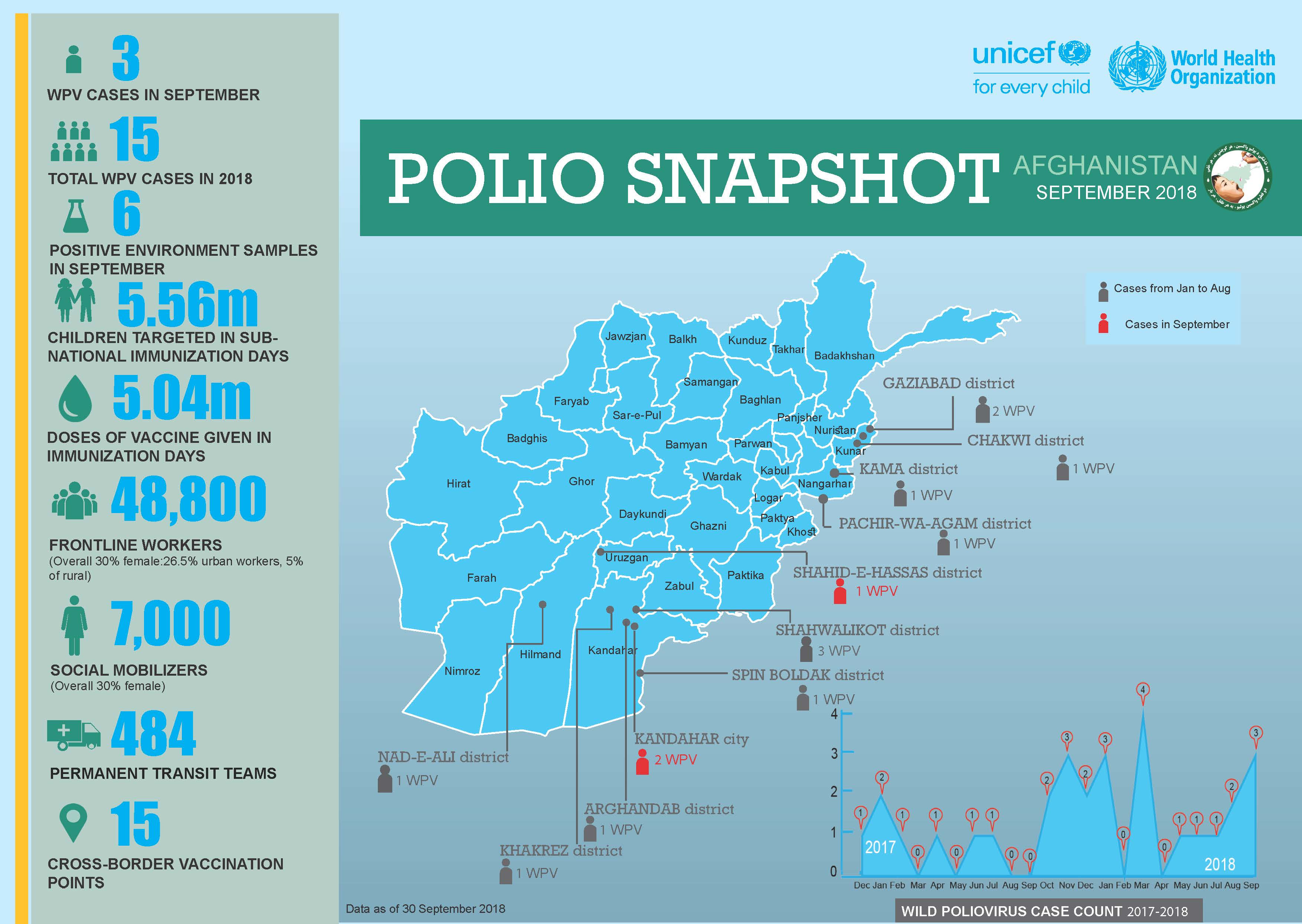
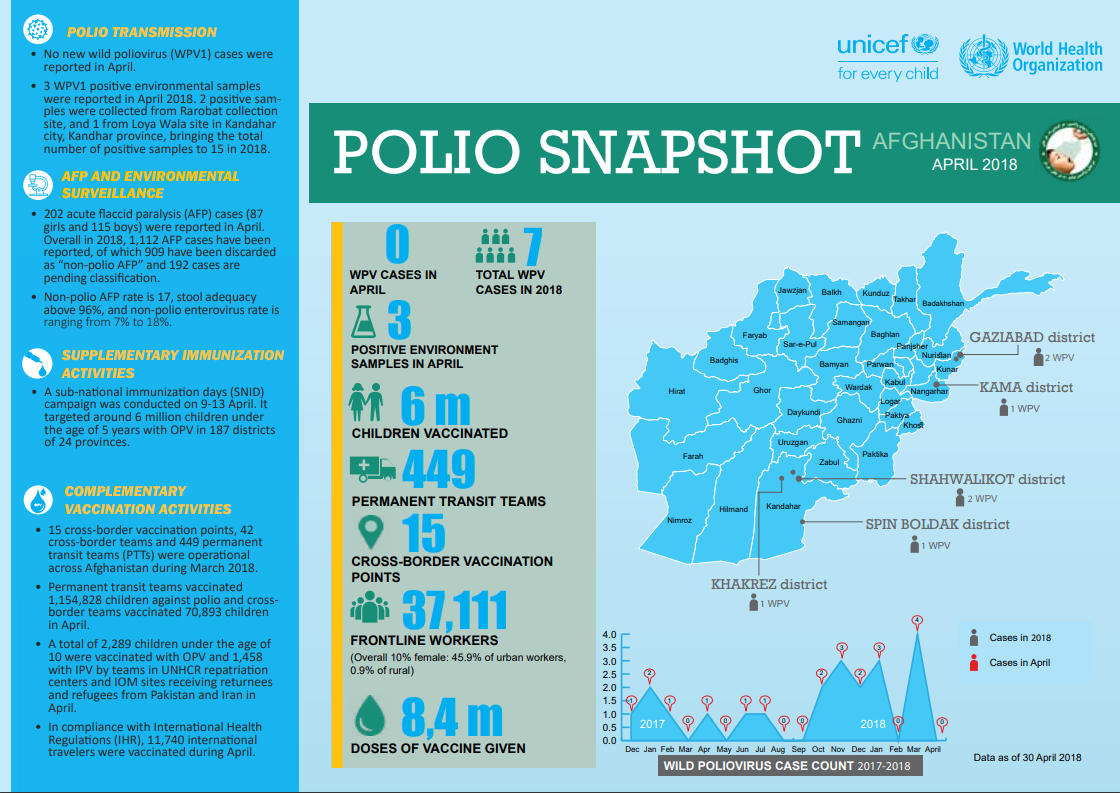
3 new wild poliovirus (WPV1) cases were reported in September 2018.
In the September Sub-National Immunization Days, 5.6 million children under the age of five were targeted.
484 permanent transit points (PTPs) were operational across Afghanistan during September 2018.
This is southern Afghanistan. A place characterized by a rich, diverse, but often complex history. Enveloped by mountains, this part of the country has seen years of conflict which have left hospitals under-resourced and health services shattered. Children face many challenges – as well as conflict and poverty, southern Afghanistan has the highest number of polio cases in the world.
In this difficult environment, the virus can only be defeated if every child is vaccinated.
Afia (not her real name), who is nineteen years old, is one of over 70 000 committed polio workers in Afghanistan, supported by WHO and UNICEF. Last month, she and her colleagues vaccinated 9.9 million children and educated thousands of parents about vaccination across the country.
The polio eradication programme comprises one of the biggest female workforces in Afghanistan: a national team, all fighting polio. Some women work as vaccinators, whilst others, like Afia, are mostly engaged in education and social mobilisation efforts. The polio programme gives women culturally-appropriate opportunities to work outside the house and engage in their community, speaking to parents about the safe, effective polio vaccine, and answering their questions. Often, women vaccinators offer other kinds of health advice, including recommendations for good child and maternal health.
To be a good vaccinator and educator, women must be committed to better health for all, with strong communication skills. They must also be organized to ensure that every child is reached during the campaign.
Afia says that if she wasn’t eradicating polio, her parents would expect her to give up her education and get married. Her younger sisters look up to her, excited to work in the polio eradication programme when they are old enough.
Her job is very important to protect all children. Afghanistan is just one of three countries – the others are Nigeria and Pakistan - that have never interrupted poliovirus transmission.
Women can vaccinate children who might otherwise miss out. Culturally, male vaccinators are unable to enter households to administer vaccine, causing difficulties if young children are asleep or playing inside. Their freedom to enter homes and give the vaccine to every child is one reason female polio workers are so critical.
Afia started work at 7 am, and is now walking home ten hours later with a young boy she has just vaccinated. Her purple burka stands out against the sand as she goes home to tell her parents and siblings about her day.
Afia feels positive about the future of polio eradication in Afghanistan: “We have a duty to protect our children, and I won’t stop working until every child is protected.”
Women have a right to participate in all aspects of polio eradication. Removing barriers to women’s full participation at all levels is a key goal for the Global Polio Eradication Initiative (GPEI). To learn more, see the gender section of our website, and read the GPEI ‘Why Women’ Infographic.
How do vaccinators ensure that every child is reached?
Every child needs to be vaccinated to protect them from poliovirus. To achieve this, detailed plans are prepared for vaccination teams. The aim is to find each child under 5 years of age – in Afghanistan, that’s around 10 million – and to reach them with vaccines.
A heavy steel gate opens on a quiet suburban street in central Herat. The city lies in a fertile river valley in Afghanistan’s west, an area rich with history. Over the centuries, invaders from Genghis Khan’s army to the troops of the Timurid empire, the Mughals and the Safavids have opened the gates to rule the city once known as the Pearl of Khorasan.
Now, a far more peaceful group can be seen walking down the streets of Herat. Equipped with blue vaccine carrier boxes and drops of polio vaccine, the teams knock on one door after another to vaccinate any children they find inside. The aim is to eradicate polio in Afghanistan.
Four-year old girl Fariba peeks from behind the gate and steps out on the street, followed by her father Mashal.
Mashal encourages his daughter to open her mouth to receive two drops of polio vaccine, and a drop of vitamin A. Fariba looks at the vaccinators with suspicion, but follows her father’s guidance.
The vaccinators thank them and continue down the street.
Locating all children
In March, vaccinators in Herat gave oral polio drops to over 150 000 children.
In a country with one of the highest rates of population growth in the world and frequent population movement, it is no easy feat to tell how many children live in each province, district, village, block, house or tent.
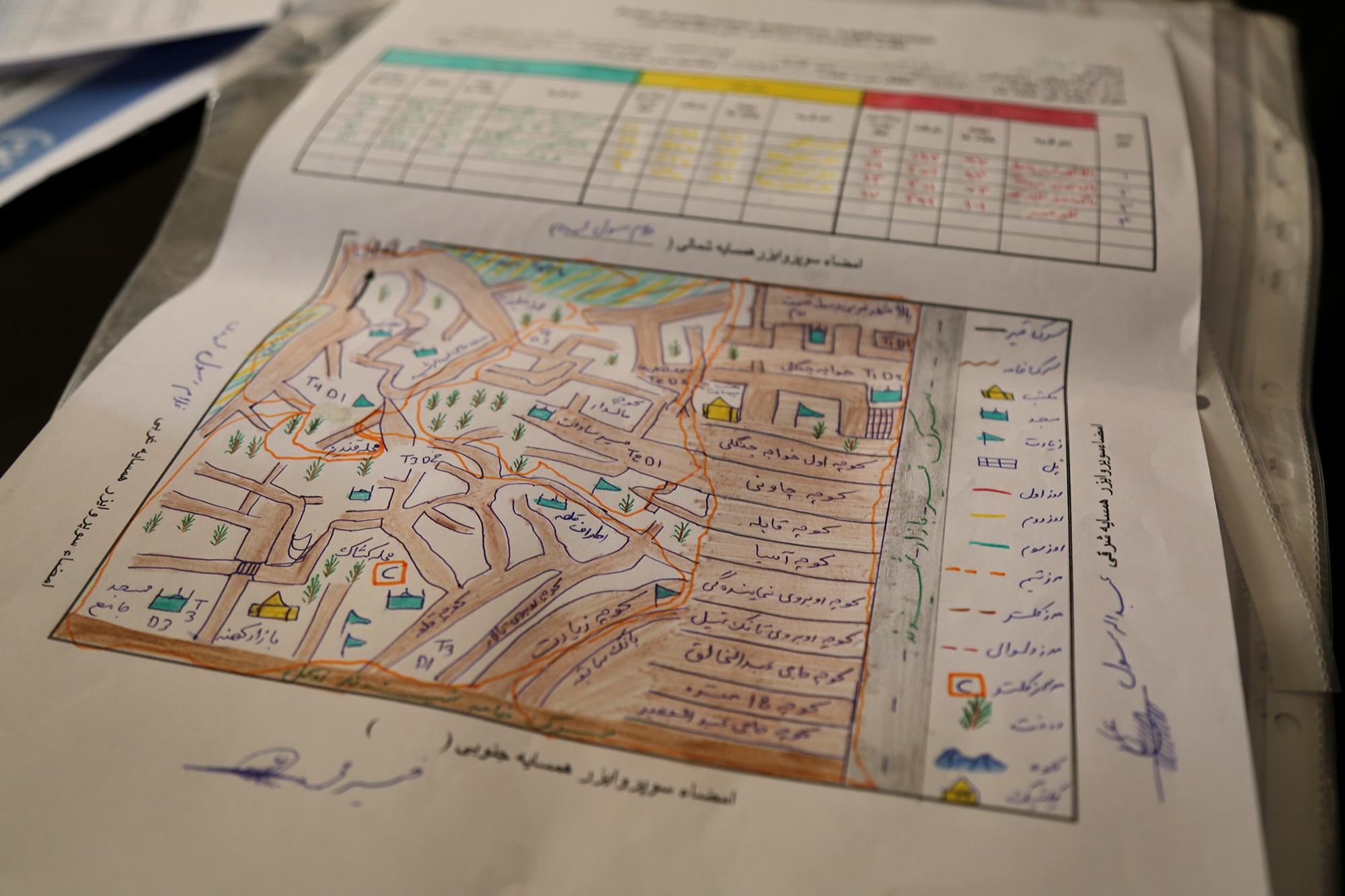
How do vaccinators know where the children in each area are located then? Through a simple but elegant guide known as a ‘microplan’. This is what the vaccinator follows: Where to start the day, how many children live on that street, which is the next house to visit?
No coincidence: Who goes where
A few kilometres from Fariba and Malik’s home, Dr Khushal Khan Zaman is sifting through printed plans on his desk at the World Health Organization office.
Dr Khushal explains that once a year, health workers physically count the houses in their area. Then they check that the plans from the previous year still match the numbers.
Campaign supervisors know the approximate number of children in each house from the last campaign. But the data is complemented by their personal knowledge. As locals, they often know of any changes in the composition of their community – where new children have been born, or the location of nomadic groups who have settled in the area.
This helps keep the plans accurate. For instance, if a nomadic group has stayed in an area for a longer time, their tents may be added to the microplans. For shorter stays, a separate checklist is used instead to monitor nomadic population movement. This improves the programme’s ability to trace and reach every child with vaccines, even if they are on the move.
Once the plans have been updated, teams of vaccinators are assigned to visit specific homes on a particular day during the upcoming campaign.
The final plan indicates not only the numbers of houses and children, but also details on how many related items are needed for each team: vaccine vials, vaccine carriers, ice packs (to keep the vaccines at optimum temperature), chalk, tally sheets, pens, leaflets, finger markers, plastic bags and scissors.
This is a contrast to a few years ago, when the plans listed only the name of the area with the estimated number of children to be vaccinated. The newer plans include even the smallest houses, and information on the closest mosque and local elders.
“It needs to be clear to everyone, which team is responsible for which area. We mark where the teams start and which direction they take using arrows,” Dr Khushal explains.
And it is no coincidence who goes where. To ensure that parents allow their children to be vaccinated, vaccinators may be allocated parts of their community that they know well, to increase trust when they deliver the vaccine.
Children like Fariba might not understand yet why the vaccine is important, but their father does. When vaccinators knock, it is not chance that brings them, but care and commitment.
In March:
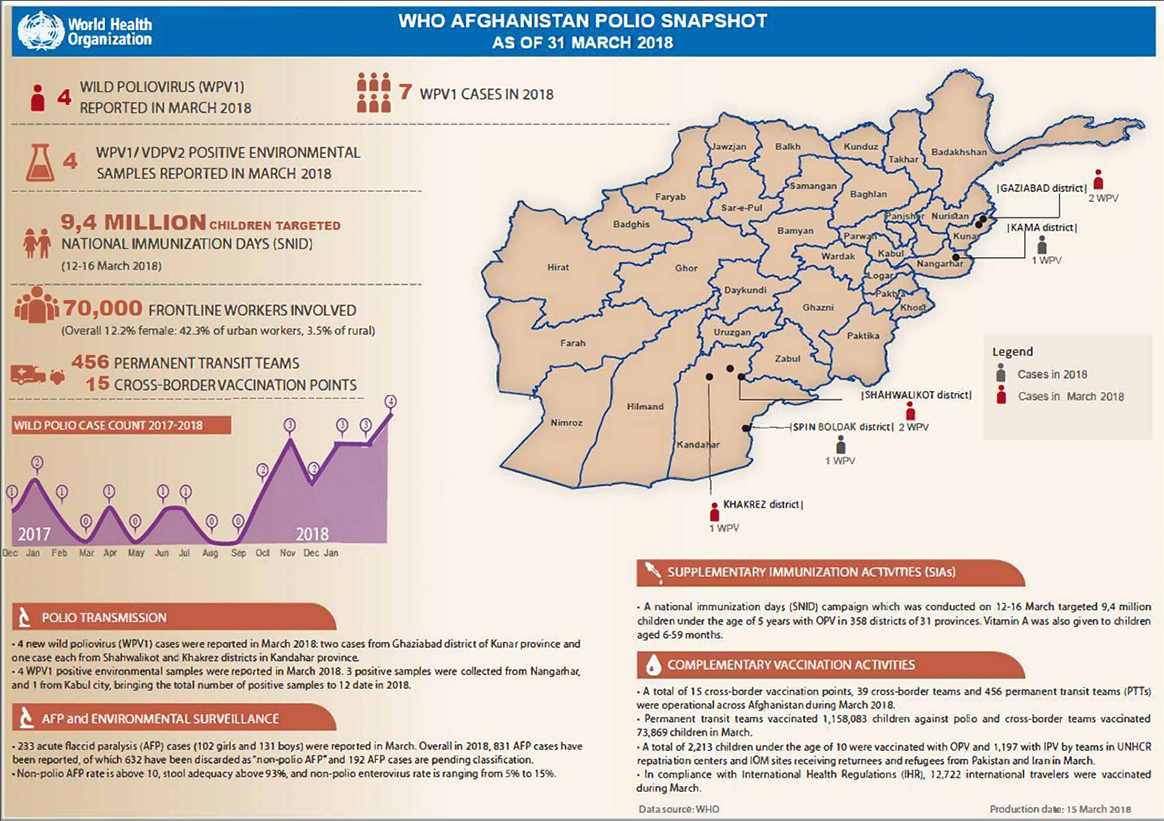
Four cases of wild poliovirus type 1 (WPV1) were reported, two cases from Ghaziabad district of Kunar province, and one case each from Shahwalikot and Khakrez districts in Kandahar province.
4 million children under five years of age were targeted during national immunization days in 358 districts of 31 provinces.
Permanent transit teams successfully vaccinated 1 158 083 children against polio, whilst cross-border teams vaccinated 73 869 children.
Last month, Canada signed a generous pledge of Can$ 100 million to help eradicate polio in Afghanistan as well as in the two other endemic countries, Nigeria and Pakistan, and to continue to protect many polio-free countries. The pledge was announced by the Honourable Marie-Claude Bibeau, Minister of International Development and La Francophonie, at the 2017 Rotary International Convention in Atlanta.
In addition to previous donations of approximately Can$ 650 million, this most recent funding consists of Can$ 30 million to WHO and UNICEF to support programme activities in Afghanistan, and Can$ 70 million of flexible funding that can be used to support vaccination campaigns, rapid outbreak response, poliovirus surveillance and other critical eradication strategies and activities to reach every last child worldwide with a safe vaccine.
This latter funding is especially valuable to the programme, as it will help sustain the priority areas of work that make global polio eradication possible. In 2017, there were 22 cases of wild poliovirus reported worldwide, from only two countries, Afghanistan and Pakistan. In Nigeria, wild poliovirus was last detected in 2016. However, since 2001, there have been wild polio outbreaks in 41 countries that were previously polio-free.
Flexible funding, such as that provided by Canada, is critical to allow the programme to react quickly to the most urgent needs, successfully stopping each outbreak, and ensuring that every child is protected from polio worldwide.
Minister Marie-Claude Bibeau used the signing as an opportunity to underline Canada’s ongoing commitment. “Canada has been a supporter in the fight against polio from the very beginning and we are committed to seeing it through to the end,” she said. “Keeping the momentum is key, particularly in Afghanistan, Pakistan and Nigeria, where polio still exists. Canada remains committed to ensuring every child is immunized, particularly girls, who continue to face barriers.”
As a champion of feminist development, Canada has particularly emphasized the role played by women in the programme, from the front lines, to programme management and political leadership. Polio eradication moreover forms a crucial part of Canada’s “Right to Health” commitment, and has the potential to become one of the first tangible outcomes of the UN Sustainable Development Goals.
Akhil Iyer, Director of the Polio Eradication Programme at UNICEF said, “Whilst polio exists in the smallest geographic area in history, this includes some of the most dangerous and difficult-to-reach parts of the world. Canada’s long-standing political and financial commitment helps our dedicated health workers, mostly women, go the extra mile and vaccinate every child to build a polio-free world.”
With this funding and ongoing support, Canada is striving to protect every girl and boy child. In doing so, Canada is making history.
The funding is also a testament to the major role played by the Canadian people at every level of the polio eradication programme. To date, Canadian Rotarians have raised and contributed more than US$ 52 million to eradication efforts, whilst Canada’s citizens have played an important role in tracking progress and publically voicing their support to end polio through the Scientific Declaration on Polio Eradication, and the One Last Push Campaign.
Michel Zaffran, Director of the Polio Eradication Programme at the World Health Organization said, “The ongoing support of Canada is fundamental to the programme’s success. With their global advocacy in international forums such as the G20 and G7 and their strategic and high quality support in Afghanistan and across the world, we can ensure that polio is eradicated forever.”
Canada’s contribution comes at an important time for the programme, in the run up to the 2018 G7 Summit. Previous summits have recognized polio eradication efforts, noting that programme assets also help to strengthen other aspects of health and development. This year, the Presidency is held by Canada, the first country to place polio eradication on the G7 agenda.
The Global Polio Eradication Initiative partners extend their profound gratitude to the Government and to the citizens of Canada for their tremendous support and engagement to end polio globally.
In March, the Afghanistan polio eradication initiative conducted its first nation-wide immunization campaign for polio eradication in 2018. In just under a week, around 70 000 workers knocked on doors and stopped families in health centres, city streets and at border crossings to vaccinate almost ten million children. What an incredible achievement.
But what does a huge campaign like this take?
We had a look behind the scenes and followed the week in Herat, western Afghanistan. See what the campaign looked like from beginning to end through this photo essay.
First there are the vaccines. Throughout the year, millions of doses of vaccines are stored in cold rooms across the country, ready to be used in immunization campaigns. Here, cold chain manager Ghulim Said shows oral polio vaccine vials − the primary vaccine used for polio eradication − which are stored in the Herat regional EPI vaccine storage facility.
Before each vaccination campaign, the polio programme draws detailed maps of where each team will head. These maps are called “microplans” and they show streets, landmarks and each house that vaccinators must visit during the campaign days.
A week before vaccination begins, polio workers start preparing. For this campaign, more than 70 000 volunteer vaccinators and other polio workers were selected and trained in vaccination, finger marking and campaign monitoring. In Herat, students Jami Mansoora (left) and Asma Hakimi (right) were trained as campaign monitors.
One day before the campaign, vaccines and other supplies were picked up from storages to be taken to the teams. These vaccines were taken from Herat regional hospital to a nearby district. They were kept in cold boxes to maintain vaccine quality.
To mark the start of the week-long effort, inauguration ceremonies were held across the country. Herat provincial governor Asef Rahimi vaccinated local children during one such ceremony.
On the first day of the campaign, banners were hung on roadsides, mosques, and health centres all over the country announcing the campaign and encouraging parents to vaccinate their children. This banner was hung on the side of a busy street in Herat city.
In the morning, the blue boxes used to keep vaccine vials cold were packed and picked up by the vaccination teams. Shireen Gul Azizi packed her bags before leaving for the day’s work. She works as a supervisor and manages three vaccination teams.
With the teams on their way, vaccination began. They walked from door to door, knocked and gave two drops of polio vaccine to every child they could find.
Ali Yaser, age 4, was vaccinated on the first day of the campaign in Herat city. All vaccinated children were also given drops of vitamin A to boost their immunity.
In addition to the house-to-house teams, mobile and transit teams worked across the country to reach any children on the move. At the border crossings, travellers were stopped and their children vaccinated. At these points, all children under ten years old are vaccinated. Mohammed Hussain Farhang, age 6, was returning from a holiday in Iran with his family. At Islam Qala border crossing vaccinator Bashir Ahmad gave him two drops of polio vaccine. He found finger-marking funny and couldn’t stop giggling.
During the campaign week, mobile teams also vaccinated children on the streets and outdoor markets. Farzad, age 16, was working by himself in the centre of Herat. In a single day, he vaccinated tens of children.
Every evening after the rounds, the vaccinators and cluster supervisors got together for a meeting to discuss any problems that might have been encountered during the day’s work.
On Thursday, three days into the campaign, the vaccinators took a break and collected numbers on how many children had not been home or had missed vaccinations for other reasons. Detailed plans were drawn and maps created showing each team which houses still needed to be revisited on the last day.
In some places, more vaccines were needed. Rickshaw driver Khalil Ahmad played his part in ensuring that every team had enough vaccines, driving more supplies to a neighboring district for the final revisit day.
On the morning of the last campaign day, cluster supervisor Ahmad Rashid examined his map to see where the five vaccinator teams he managed would be heading. He knew the revisit day was important during every campaign: this was the chance to reach every last child in his area.
One of Ahmad Rashid’s teams, vaccinators Sumaya Hakimi (left) and Sohaila Hamidi (right), started working at eight in the morning. From their maps they could see that they had missed 36 children during the week. By 11 a.m., they had already found 30 of the children at home and had vaccinated them.
Success! Moheburrahman, age 3, was not vaccinated earlier in the week when the team visited, as his mother was worried about the vaccine’s safety. The team talked with the family again, carefully explaining why the polio vaccine is so important, and taking time to discuss their concerns. Reassured that the vaccine is safe, little Moheburrahman’s mother allowed the vaccination to go ahead.
One last child protected against paralysis. Little one-day-old Fatima received her first ever vaccination on the last day. She could not be vaccinated earlier, as she had not been born yet.
After the campaign, more than 1 800 independent monitors were deployed to find any missed children and record the reason they were missed. This information will help preparations for the next campaign.
In a local health centre in Herat, Najibullah Mohammadi conducted a finger-marking survey to check if every child had a little blue pen mark on their fingers. On little babies the mark was drawn on the ear – an easy way to show they have been vaccinated whilst keeping them wrapped up warm. 45-day-old Rokshana was found to be vaccinated.
Rokshana and every child deserves a healthy, polio-free life. Thanks to the work of the thousands of volunteers and polio workers, Afghanistan is one step closer to eradicating the disease.
The Afghanistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Afghanistan.
In February:
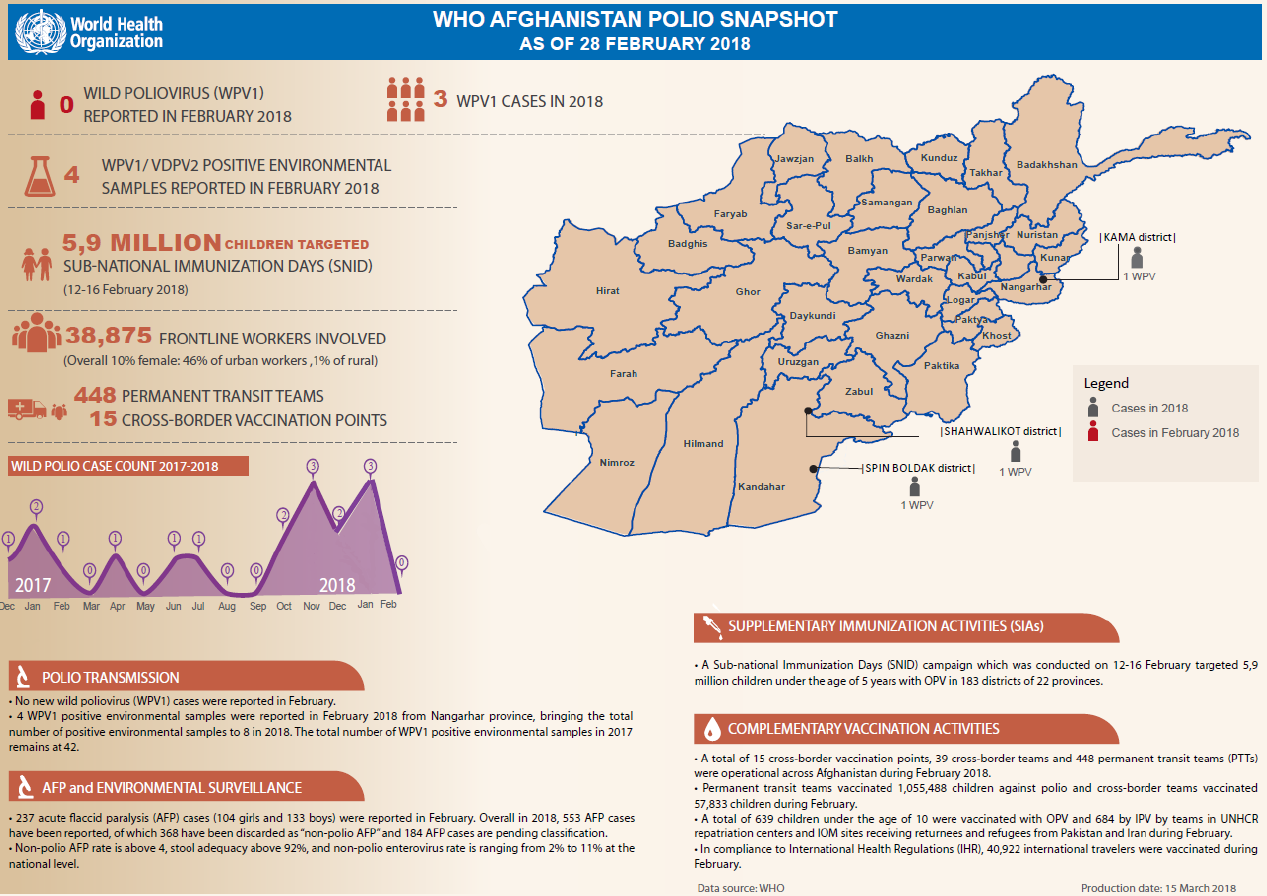
No new cases of wild poliovirus type 1 (WPV1) were reported.
5.9 million children under five years of age were targeted during subnational immunization days across 22 provinces.
Permanent transit teams successfully vaccinated 1 055 488 children against polio, whilst cross-border teams vaccinated 57 833 children.
In eastern Afghanistan, one family is helping to vaccinate every last child in their community
Zahed, his daughter Sahar, and son Mohammad all work together. But they are not working for themselves, they are working to eradicate polio.
The family lives in an indigent village in eastern Afghanistan with a diverse community. It is close to the border with Pakistan and many residents are returnees from Pakistan, families displaced by insecurity and nomads passing through. With a population that is often on the move, it is a community with high risk of poliovirus transmission – making it extremely important to vaccinate every child.
Zahed’s family are well-known. Each month, they knock on doors giving free vaccinations and educating their community about the virus.
Although sometimes they don’t have doors to knock – only tents. Known in Afghanistan as Kuchis, nomads are particularly vulnerable to polio, because they move seasonally and often miss vaccination campaigns. Historically underrepresented and often neglected, they are also isolated from health services.
Nomads at risk
Laden with water jugs, cooking equipment and clothes, the Kuchi travel with their livestock and move between provinces depending on the climate. Their goats, sheep and camels are often exchanged or sold for grain, tents and other essential items. There are an estimated two million nomads in Afghanistan.
Over 120 nomad families with 194 children under the age of five recently arrived in Zahed’s village from shelters along the Kabul River. They come in the winter because it offers warmer, more fertile ground for their animals to graze. They return to Kabul and Bamiyan during the spring, when the land is more arable.
To eradicate polio in Afghanistan, every child must be vaccinated – including the nomads. And this is exactly what Zahed’s family are doing. They go to each tent, and ensure every child is protected against polio. Last week, Zahed’s 20-year-old son Mohammad vaccinated 719 children, including nomads. “My community are happy with my service. I’m young, and it is a privilege to make a difference,’’ says Mohammad.
The family is not only protecting children, they are also contributing to community cohesion and bridging divides between nomads and residents. The challenge, however, is continuing to vaccinate nomads when they are on the move.
The motivation of Zahed’s family is impressive, but it is not always easy. A handful of people in the village reject the vaccine because they think that it is unsafe or not halal – permissible in traditional Islamic law. But watching an entire family working to eradicate polio helps break misconceptions. At the start of each vaccination campaign, Mohammad gives one of his own children the vaccine to prove that it is safe.
Becoming advocates
Zahed’s family have turned almost all the families who were refusing the polio vaccine into advocates for vaccination. Mohammad was already a prominent member of the community and was previously given a ‘Turban’ – headwear used to recognize a person who makes decisions on behalf of their community and country – to honour his relentless work to improve water, sanitation and development in his village. Now his role as a polio eradication ambassador is developing trust and increasing acceptance of the vaccine.
In 2017, three polio cases and 14 positive environmental samples were reported in eastern Afghanistan. A positive sample indicates that the polio virus is present, and that children with low immunity are at risk of contracting the disease. The first polio case of 2018 was also reported in eastern Afghanistan, making it an urgent priority location for nationwide eradication.
In the village, polio has almost been eradicated. But this is not enough for Zahed’s family. As they prepare for their next vaccination round, they are determined not to stop their work until everyone in their community – wherever they are from – is safe from polio.
Vaccinating every child, every time Haroon, 3, was vaccinated for the second time in two weeks. WHO / Tuuli Hongisto
In Afghanistan, frontline health workers explain to parents why the polio vaccine must be delivered multiple times
“It’s easy for the others, they are young and strong!” laughs Hamida. She has just climbed hundreds of steps to the top of a long and steep staircase on the side of one of Kabul’s many hills. Together with her colleagues Mohib and Khalid she works as a part of a polio team vaccinating children in their community. Today, the team started at 8 am, and they have now been walking up and down the hill for three hours. No wonder she is tired.
So far, the group has visited 50 families and vaccinated 110 children. They have 30 more to go today, and, in the next three days, they will visit a total of 233.
The team’s role is not only to vaccinate the children but to also to educate people about the life-saving polio vaccine and its importance. It is not always an easy job.
“Last time we visited was only two weeks ago, so some parents have been asking why we are visiting again. I have explained to everyone that the vaccine is beneficial for the children and that children need to be vaccinated every time we visit to be protected.”
It is the first day of a vaccination campaign, which aims to immunize over 6 million children against polio in Afghanistan.
Today, thankfully, all families have accepted the vaccine from this team.
Last push to eradicate polio in Afghanistan
Afghanistan is one of the last countries in the world where wild poliovirus still circulates, and has the highest number of children paralyzed by the virus.
In 2017, there were a total of 14 cases and, so far in 2018, there have been three confirmed cases. In recent months, the virus has been found circulating in southern and eastern regions.
WHO Afghanistan polio programme manager Dr Hemant Shukla is confident that with stepped-up efforts, the circulation can be stopped. “Afghanistan has stopped transmission in the past in all areas, but not at the same time. We are confident that by following correct strategies, focusing in the right areas and by coordinating our efforts with neighbouring Pakistan, we can stop the transmission”.
To answer to the challenge, the Polio Eradication Initiative has stepped up efforts to detect any viruses in the environment. The programme is taking special steps in the eastern and southern regions to reach all children with the vaccine every time the vaccinators pass by, as these are very high risk areas for polio transmission, with people moving in and out of neighbouring Pakistan. Special outreach tactics are concurrently aiming to reach and immunize ‘mobile populations’, such as nomadic people, who are at high risk of contracting polio.
The oral polio vaccine is effective as it not only protects children from contracting the virus, it also prevents them from carrying it in their intestines. Several doses – spaced apart – need to be given to build sufficient immunity, especially in areas where poor nutrition can weaken immune systems.
During the low transmission season, the Polio Eradication Initiative conducted two campaigns – in January and February – in order to vaccinate children in high risk and very high risk districts in quick succession so that the vaccine would have a maximum effect.
In March, 10 million children across the whole country will be vaccinated – that’s every single child under the age of five years.
In Kabul, one by one the team marks their tally sheet with numbers and ages of the children and takes note whether all the children of the household were present.
One of the children vaccinated today is three-year-old Haroon, who stands outside his family’s home. His mother Nadia peeks through the gate. She has six children, and Haroon is her youngest.
“Haroon was just vaccinated two weeks ago, but I know it is important to vaccinate children every time”.
The team marks this household vaccinated for today.
In four weeks, Nadia will open up her door when the vaccinators knock again.
The Afghanistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Afghanistan.
In January:
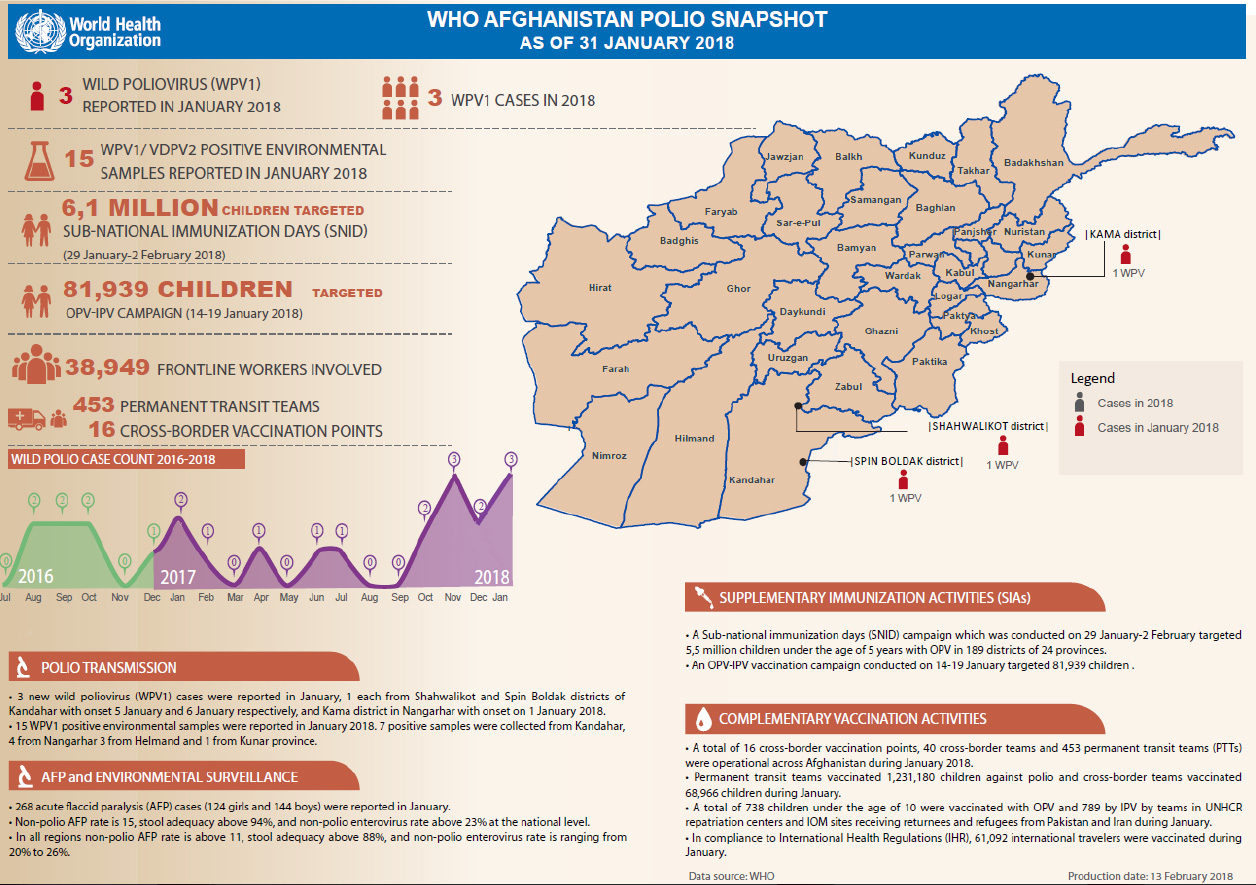
Three new cases of wild poliovirus (WPV1) were detected, two from Kandahar province, and one from Nangarhar province.
6.1 million children under five years of age were targeted during subnational immunization days across 24 provinces.
Permanent transit teams successfully vaccinated 1 231 180 children against polio, whilst cross-border teams vaccinated 68 966 children.
The poliovirus remains in just a few small pockets around the world. However, these final hiding places are some of the most challenging settings on earth in which to eradicate a disease. Finding and stopping a virus whose special power is staying hidden is no mean feat, especially in remote or inaccessible places.
Disease detectives around the world are working tirelessly to find every last virus in these hard to reach places. Some areas are vast and sparsely populated, such as the broad plains and river beds making up areas of the Lake Chad region. Others are densely packed residential areas of Afghanistan, where security issues can sometimes make immunization difficult. In areas of Syria, civil war continues to rage through towns, communities, and families. Yet these challenges are not enough to stop the surveillance system.
Community-based surveillance
In such difficult environments, the polio surveillance system must overcome numerous challenges to ensure that the poliovirus is tracked. Experts look for the virus in children with symptoms of acute flaccid paralysis and also in water samples from sewage systems in high risk areas.
For Dr Arshad Quddus, Coordinator for the detection and interruption of poliovirus at WHO headquarters, the key to overcoming the challenges facing polio surveillance is tapping into communities. Illustrating his point, he draws a circle on a piece of paper, placing a dot in the middle. In Afghanistan, he explains, that dot represents a surveillance focal point, based at a District Health Centre or hospital. The circle extending from them is their information network – a collection of mullahs, healers, health-care providers, teachers, parents and other surveillance recruits – who have been trained to spot cases of acute flaccid paralysis in their community that could turn out to be polio.
Each volunteer is given a book in which to write down the information they find, and a phone number to call. If they come across a case in their local community, they must ring their focal point, setting in action a series of events that will allow the child to be examined, stool samples to be taken from them to be tested in the laboratory for polio and their close contacts tested.
Overcoming challenges
The system may seem simple, but insecurity, weather and challenging landscapes can be obstacles. In Afghanistan, the programme has developed creative ways to ensure that nothing stands in the way of the surveillance system being able to work as it needs to. In most cases, following the reporting of a case of acute flaccid paralysis, health workers will visit the child’s home to inspect them, and collect stool samples from the child to send for lab testing for the poliovirus. However, if the area is inaccessible, the child and their caregivers are transported to the nearest hospital in a safe area for inspection.
For Dr Quddus, the success of this system in Afghanistan is clear: “We have regular reports of where the poliovirus is circulating in difficult and hard-to-reach communities and this shows us we are being successful, despite tremendous challenges.”
Surveillance in conflict zones
These diverse methods also strengthen surveillance in countries where the security situation is rapidly changing. In Syria, the health-care system has been weakened due to conflict, with many of those at the heart of the polio surveillance system displaced. By building new networks in camps for internally displaced families where communities are created by proximity, and recruiting surveillance volunteers at the key points of entry and exit into the worst of the conflict zones, the polio surveillance system ensured that an outbreak of circulating vaccine-derived poliovirus in 2017 was rapidly identified and an outbreak response launched. The programme also thought outside of the box in Borno, Nigeria, by training medical corps being deployed to reach conflict-affected populations to spot signs of the virus.
The polio surveillance system is strengthened by a mixture of community, adaptability, and fierce commitment to finding every last trace of virus. These are the lessons learned that help find the virus everywhere, from urban districts of Afghanistan, to hard-to-reach areas of Nigeria. For Dr Quddus, “It is the individuals on the ground willing to give their all that will enable us to achieve eradication. The surveillance system is the eyes and ears of polio eradication, showing us where to focus our best efforts to vaccinate every last child.”
Environmental sampling from an open drain in Kabul city in August 2017. Samples are generally collected in the early morning when there is a higher flow of sewage. WHO/S.Ramo
Afghanistan is increasing the drive to track and understand the movement of the polio virus by expanding environmental surveillance – collecting and testing sewage samples for poliovirus in the laboratory – to all regions. At the end of 2017, a new environmental sampling site became operational in Kunduz province, becoming the 20th site since the collection and testing of sewage samples for poliovirus began in Afghanistan in 2013, with WHO support.
In 2017, 317 sewage samples were collected from all sites, and 30 of these showed that the poliovirus was present. This insight means that the polio eradication team knows where the virus is, without relying on the identification of paralysed children. Given that for every one polio victim there can be hundreds of ‘silent’ cases – children infected but with no symptoms – improved environmental surveillance is like giving the programme x-ray glasses with which to find and track the virus.
Rolling out environmental surveillance
“We began the expansion of the surveillance system in the most high-risk provinces of Kandahar and Helmand in the south where we have also doubled the frequency of sampling to every two weeks to increase the chances of picking up the virus where it circulates,” said Dr Hemant Shukla, Director of the Polio Programme at WHO Afghanistan. “Our next priority was to establish additional sites in the eastern region, and now environmental surveillance has expanded to nine provinces, covering all regions in Afghanistan.”
The importance of good surveillance
A sensitive surveillance system remains the cornerstone of polio eradication efforts. Environmental surveillance helps to determine possible routes of transmission and enabling a swift response to stop further spread of the virus.
Environmental surveillance complements acute flaccid paralysis (AFP) surveillance which currently consists of a network of over 28 000 reporting volunteers and focal points, including health workers, teachers, religious leaders and traditional healers. Volunteers detect and report children showing signs of polio, such as floppy or weakened limbs with rapid-onset of paralysis. Finding and stopping every last strain of the poliovirus requires both sensitive AFP and environmental surveillance.
Technical team from WHO and the Ministry of Public Health packs a sewage sample to be sent for further testing to the regional laboratory in Pakistan. WHO/S.Ramo
Using surveillance to stop polio
In 2016, WHO and the Ministry of Public Health conducted a comprehensive assessment of existing environmental sampling sites, identifying new sites for expansion. Since the beginning of the year, WHO has supported the establishment of four new sampling sites to further boost Afghanistan’s surveillance capacity.
“Strengthened environmental surveillance has helped us to identify and locate wild polioviruses when they are circulating. Whenever virus is found in the environmental samples, WHO supports a strong response in that area, which includes vaccinating all target-age children to boost their immunity levels to protect them from polio and further strengthening routine immunization services in the area,” explains Dr Ali Ahmad Zahed, Surveillance Officer at WHO Afghanistan.
Expanding the surveillance system
Before each new site is established, WHO conducts a two-day theoretical and practical training for environmental surveillance personal, demonstrating how samples are properly collected, labelled, packed, stored and transported into the laboratory for testing. After each sample is collected from a sewage site, it is frozen and sent to the regional laboratory in Pakistan for further testing and analysis, utilizing a reverse cold-chain process to ensure the virus does not denature in the heat.
Afghanistan is closer than ever to stopping poliovirus transmission as the virus is currently cornered into small, security-challenged parts of the country. Thirteen cases of acute flaccid paralysis caused by polio have been reported to date in 2017 from Kandahar, Helmand, Kunduz, Nangarhar and Zabul provinces. In 2016 Afghanistan reported 13 wild poliovirus cases from four districts, compared to 20 cases from 16 districts in 2015.
“Since environmental sampling started in 2013, we have collected and tested over 756 sewage samples. Our AFP surveillance network expanded by 20% last year alone. Afghanistan’s polio surveillance system is the strongest it has ever been. If poliovirus is circulating anywhere in the country, we will be able to trace it and stop it in its tracks,” says Dr Zahed.
Follow the workday of female polio vaccinators through this photo story.
WHO / Tuuli Hongisto
Zainab (left), a female polio vaccinator from Afghanistan, meets with one of her vaccinator teams. This team has already vaccinated 49 children today, and it is only 9.30 in the morning.
WHO / Tuuli Hongisto
Women like Zainab are on the frontline of polio eradication, ensuring vaccines reach every child, every time. A five-year-old boy, Waris, is vaccinated against polio in Loya Wala, Kandahar.
WHO / Tuuli Hongisto
One of the vaccinators working with Zainab hands out red, orange and green balloons to Waris and all of the other children after marking the children’s fingers in blue marker pen to show they have received the vaccination.
WHO / Tuuli Hongisto
A girl looks on as her finger is marked after vaccination. This dot of ink will show the campaign monitors that this child is protected, and will enable them to find and vaccinate missed children.
WHO / Tuuli Hongisto
Zainab, (right), gets ready to knock on the door with her team of vaccinators. “I like to be a supervisor and have my own teams. I used to be a vaccinator in a health centre, and have been working in the polio eradication programme since I graduated.”
WHO / Tuuli Hongisto
The team marks the number of vaccinated children on a tally sheet and register book after each visit. At the end of the day, the team calculates how many children were reached.
WHO / Tuuli Hongisto
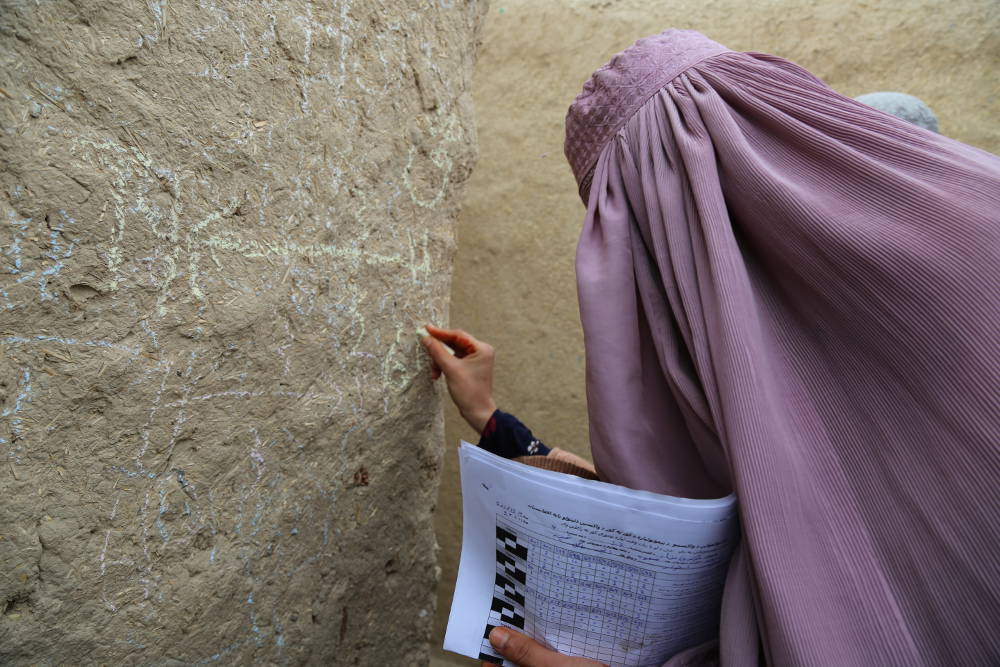
Zainab’s colleague Asma writes in chalk upon the wall of a house where they have just vaccinated several children to help vaccination campaign monitors check whether all children have been reached.
WHO / Tuuli Hongisto
At the end of the day, the teams go through their day and share any problems encountered in a meeting.
Reducing polio cases by 99.9% globally is an incredible feat, achieved through innovative strategies and years of trial and error.
While the polio eradication programme is focused on getting to zero, now is the time to make sure everything we’ve learned isn’t lost and can be used to inform future global health programmes. Just as the polio eradication effort applied lessons learned from the successful smallpox campaign to its own work, the goal is for future health programmes to understand and build on the knowledge of the polio effort.
Under a new grant from the Bill & Melinda Gates Foundation, the Johns Hopkins Bloomberg School of Public Health (JHSPH) will be working to do exactly this.
JHSPH will partner with academic institutions from around the world to document lessons and develop graduate-level courses and hands-on training clinics for public health students and professionals, including an online open course available to the public and implementation courses for managers from other health programmes.
Under the leadership of Dr Olakunle Alonge, the team at JHSPH will collaborate with a global team from public health institutions in seven countries: Nigeria, India, Afghanistan, Ethiopia, the Democratic Republic of the Congo, Bangladesh and Indonesia. This will not only ensure a balanced and diverse perspective, but also enable the exchange of public health training strategies between the institutions.
To develop the content of each course, JHSPH will be identifying “change agents” at the local, national and global levels who have expertise in polio eradication that may not otherwise be captured. This unique global strategy promises to yield coursework that speaks to the issues faced by a broad range of global health programmes and actors.
“Without an active strategy to map, package and deliver the knowledge from the global polio eradication efforts to other programs and global health actors, I’m afraid that these knowledge assets may not find any useful purpose beyond the end of the polio campaign, which could come to an end within a few years,” said Alonge.
Alonge expects to glean lessons that will apply to immunization systems, public health emergency response, primary health care, disease eradication and infectious diseases—ensuring that the polio programme continues to positively impact global health for years to come.
The Afghanistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Afghanistan.
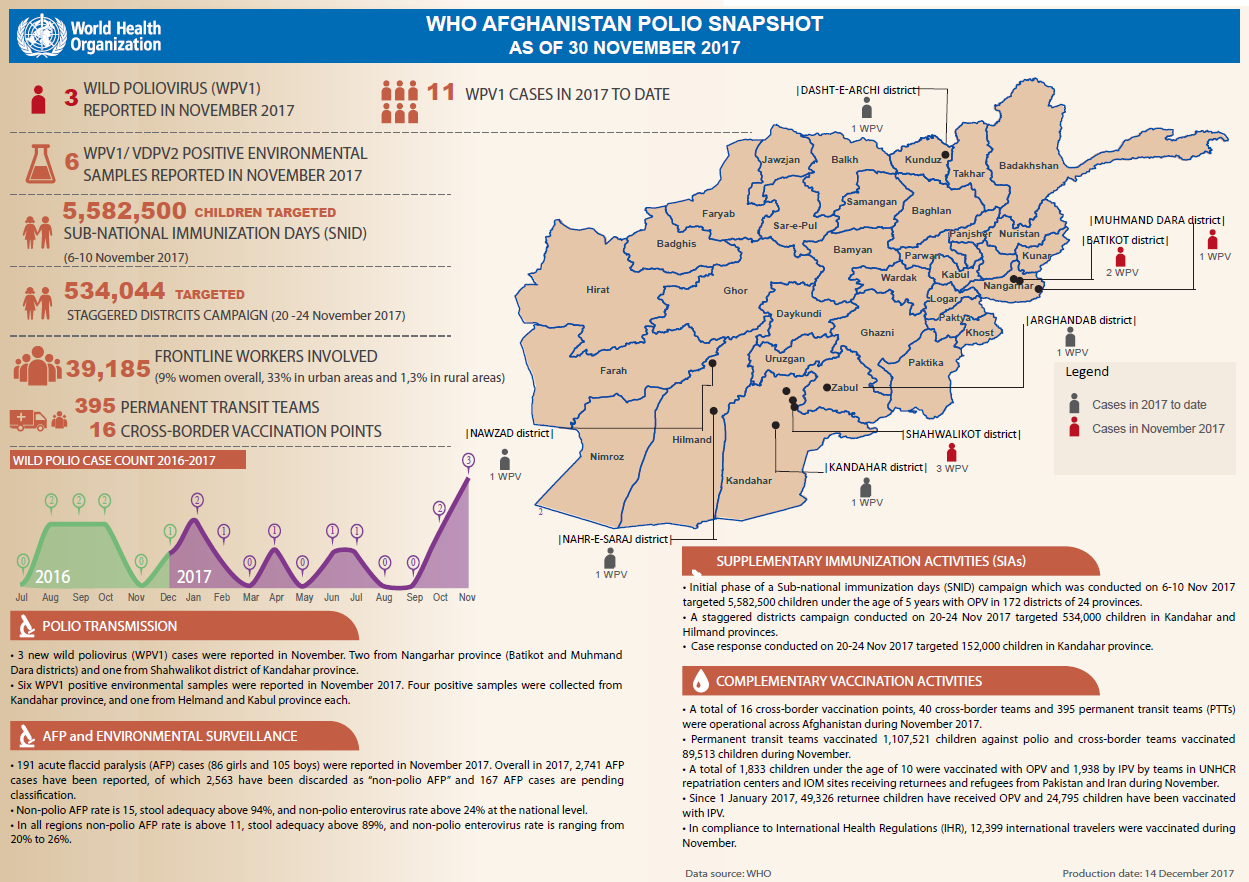
In November:
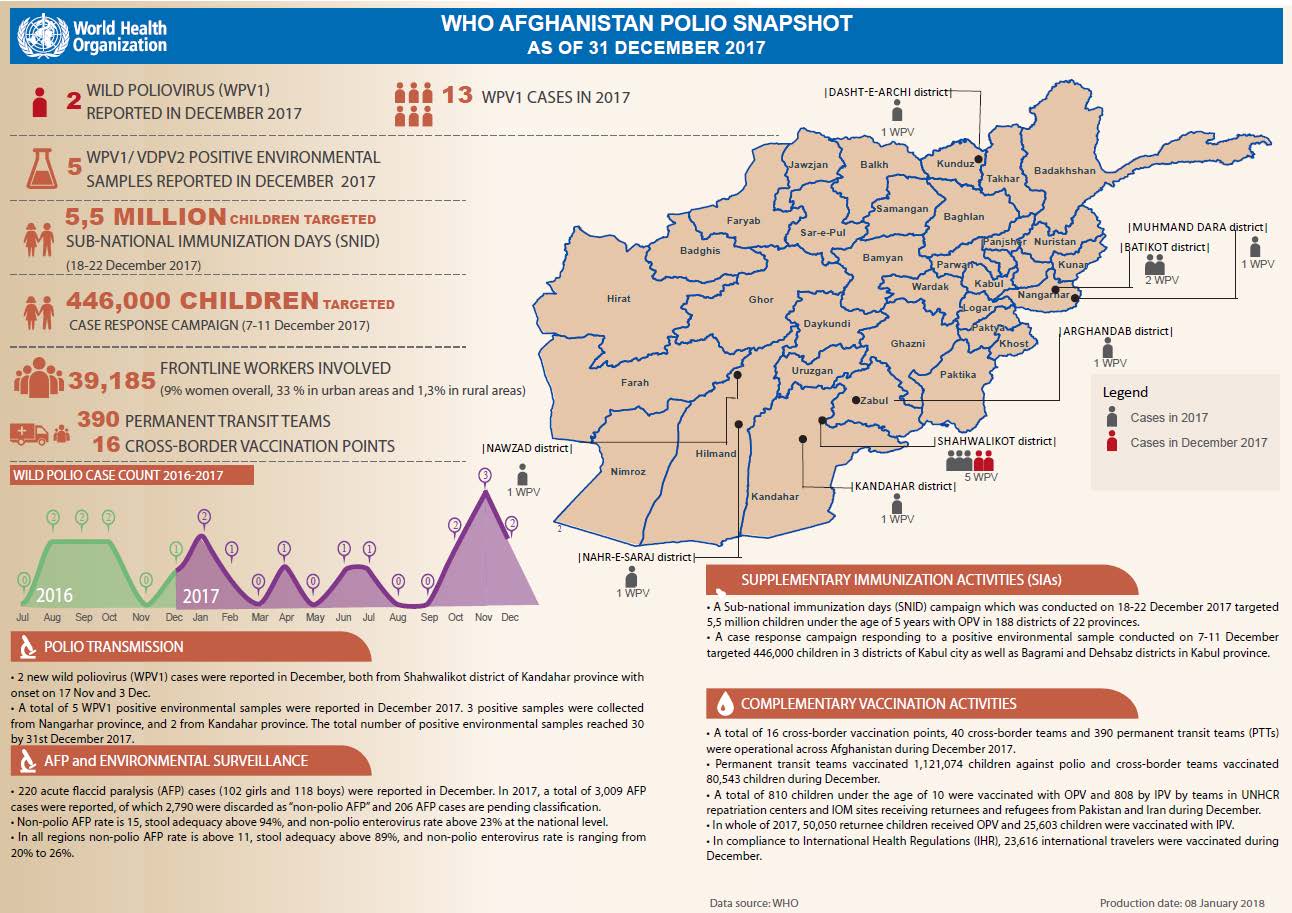
Three new cases of wild poliovirus (WPV1) were detected, two in Nangarhar, and one in Kandahar provinces.
Over 6 million children under five years of age were targeted during subnational immunization days and a staggered districts campaign.
Permanent transit teams successfully vaccinated 1,107,521 children against polio, whilst cross-border teams vaccinated 89,513 children.
The year’s end offers the chance to reflect on the polio programme’s milestones and challenges in 2017, and look ahead to what we can achieve in the coming year. 2017 saw the fewest wild polio cases in history — a total of 17 cases, or a 50% reduction from the year before—with these cases occurring in just two countries: Afghanistan and Pakistan. Yet the need to reach every last child is more important than ever, as demonstrated by surveillance gaps in Nigeria and outbreaks of vaccine-derived polio in Syria and the Democratic Republic of the Congo.
From programme strategies that helped protect progress and overcome obstacles, to commitments from donors and partners, 2017 demonstrated the resolve required to achieve a polio-free future. Accelerating progress in the new year and ending polio for good will require maintaining these political and financial commitments as well as building upon the programme’s efforts to find the virus wherever it exists.
Rooting out the virus
Throughout 2017, developments in disease surveillance – both in humans and in the environment – allowed the programme to better hone in on the virus and identify its remaining hiding places.
These innovations are building robust, sensitive surveillance networks around the world that pick up every trace of the virus and enable the programme to develop targeted immunisation responses before polio has the chance to paralyse children.
The year also came with new challenges, including outbreaks of circulating vaccine-derived polio in Syria and the Democratic Republic of the Congo, where conflict has ravaged the health infrastructure. In these communities, and others where polio still exists, difficult terrain, conflict and highly mobile populations can all stand as hurdles to vaccinating children. Yet the polio programme continues to find new and effective ways of delivering vaccines.
For example, in Afghanistan, a collaboration with a mobile circus is sharing important messages about polio vaccination with hard-to-reach populations, including those living in camps for internally displaced persons. In Pakistan, campaigns based at border crossings and train stations vaccinated children on the move who might otherwise have been missed by traditional methods. And in Syria, dedicated workers are delivering vaccines at transit points and registration centres for internally displaced persons. Thanks to these strategies, more than 255,000 children have been vaccinated in Deir Ez-Zor, 140,000 were reached in Raqqa and the programme continues to work to reach every child.
The mobile circus passed on vital health care and social messages, encouraging full immunization of every child. UNICEF Afghanistan / Ashley Graham
Renewed commitment to end the disease
Complementing these programmatic innovations were political and financial commitments that highlighted polio eradication as a priority for global health leaders. These included:
Next year, country programmes will need to continue working to ramp up surveillance, particularly in Nigeria, and reach children everywhere with vaccines. Cross-border coordination between Pakistan and Afghanistan, which has already had a huge impact in reducing cases, will continue to be critically important to stopping transmission.
At the same time, the global community is beginning to solidify plans for keeping the world polio-free once eradication is achieved. Countries are developing strategies for transitioning the infrastructure and tools that they currently use to fight polio. And the GPEI is working with global stakeholders and partners to develop the Polio Post-Certification Strategy, which will define the activities needed to keep polio from returning after the virus is eradicated.
If the remaining endemic countries continue to do all that they can to stop the virus, and if the global community continues to meet the level of political and financial commitment needed to make and keep children everywhere polio-free, 2018 will bring the world’s best opportunity yet to end the disease.
Despite focused efforts to stop the transmission of wild poliovirus in 2017, to date this year 17 cases have been reported globally; six from Pakistan and 11 in Afghanistan. During a series of meetings to review progress in the two endemic countries, which make up one epidemiological block, members of the Technical Advisory Group (TAG) on polio eradication concurred that while both Pakistan and Afghanistan continue to make progress, continued transmission threatens gains already made towards interruption.
The TAG meetings, held in Islamabad and Kabul, recognized the efforts of both countries to coordinate activities closely, focusing on clearly identifying missed children, the reasons they have been missed, and putting in place operational plans to overcome these challenges. Efforts made to adjust national emergency action plans and build on the lessons learned from previous years and other countries have been commended by expert members of the TAG and hailed as key drivers behind the momentum.
TAG however reminded the country programmes of the remaining gaps and concluded that consistently reaching and vaccinating high-risk mobile population groups is essential if Afghanistan and Pakistan are to interrupt transmission over the coming months.
Ongoing transmission threatening the end game
The greatest risk to polio eradication, according to TAG chair Jean Marc Olive, are the reservoirs that continue to harbor the virus: the northern corridor comprising of eastern Afghanistan and Greater Peshawar – Khyber in Pakistan, the southern corridor linking southern Afghanistan (Kandahar and Hilmand) with Quetta block, Balochistan province, in Pakistan and Pakistan’s economic hub, Karachi.
Recognizing the already high level of Government commitment from both countries, TAG insisted that sustained leadership at all levels in both countries would be essential for the implementation of recommendations, including maintaining coordination at the national, provincial and district levels, as well as among the bordering districts in the common corridors of transmission.
Specific recommendations for addressing areas with continued transmission included the development of joint Action Plans for the common reservoirs (northern and southern corridors) linking the two endemic countries ’ as well as to strategize for improving program implementation quality in other high risk areas as well as among the high risk mobile populations.
About the Technical Advisory Group
The Technical Advisory Group (TAG) was established to review progress towards polio eradication in specific countries, assess implementation of previous TAG recommendations, discuss planned activities and issue recommendations to address constraints facing national programmes in achieving their targets. TAG meetings are attended by country-specific TAG members, national representatives and partner organizations, both international and regional.
In Afghanistan this year, staff from the non-governmental organization Care of Afghan Families collected 420 blood samples from children under 4 at the Mirwais Regional Hospital in Kandahar province. The aim? To find out whether polio vaccination campaigns have been reaching enough children, and whether the vaccines have been generating full protection against this paralysing disease. These ‘serosurveys’ showed that immunity in Afghanistan is high – and also identified where vaccination campaigns need to reach out further.
Whenever a polio vaccination campaign takes place, a purple dot of ink is painted onto the little finger nail of every immunised child to show that they have received the lifesaving vaccine. This data is collected and allows people to monitor the campaign and know exactly where children have been reached.
Now, with more children being vaccinated than ever before, the polio eradication programme needs to know more than how many children are being reached: we need specific data on where children are being missed.
Serosurveys testing for immunity
Serosurveys are simple tests of the serum in a child’s blood, which measures their immunity (or seroprevalence) to different diseases. The polio eradication programme uses this test to see what level of protection a child has against wild poliovirus types 1, 2 and 3, allowing them to assess whether the vaccination campaigns are reaching enough children, enough times, to give them immunity.
At the Mirwais Regional Hospital, the children tested were from a diverse range of provinces. Their results were sent to Aga Khan University for initial testing, and then sent for further analysis to one of the Global Polio Eradication Initiative partners, the US Centers for Disease Control and Prevention in Atlanta. Through mapping both where they live and their immunity results, scientists at both institutions helped polio eradicators to discover the areas where a child is at most risk of being missed by vaccination campaigns.
Serosurvey results can be crucial for planning campaign strategies – making sure that every last child is reached, no matter where they live.
For Ondrej Mach, team lead for clinical trials and research in the WHO’s Polio Eradication Department, serosurveys “… are increasingly important for eradication efforts, allowing us to form an accurate picture of our progress so far, and the locations where we are being most effective.”
High immunity in Afghanistan
The Mirwais serosurvey proved that Afghanistan is closer than ever to eradicating polio, with more than 95% of children surveyed immune to wild poliovirus type 1, the virus type still circulating in some areas of Afghanistan, Pakistan and Nigeria, and more than 90% immune to type 3, which hasn’t been found anywhere in the world since November 2012. The tests also pointed to where gaps in immunity are, so that missed children can be found and protected.
These results are a strong reflection of the devoted work of polio vaccinators and community workers throughout the country, using their expertise to reach into every family, and spread awareness of the importance of polio vaccination.
As in Afghanistan, serosurveys are increasingly used in other countries where polio remains or poses a threat, to help identify the last remaining pockets of under-immunized children in high risk areas. This is especially important because with polio in fewer places than ever before, it is these unreached children that will take us over the finishing line.
By getting an increasingly accurate picture of where vaccination campaigns are operating successfully, as well as where the programme needs to renew efforts, we can move further towards the goal of reaching every child.
This helps us reach our ultimate goal – ensuring that every last child, everywhere, can be polio free.
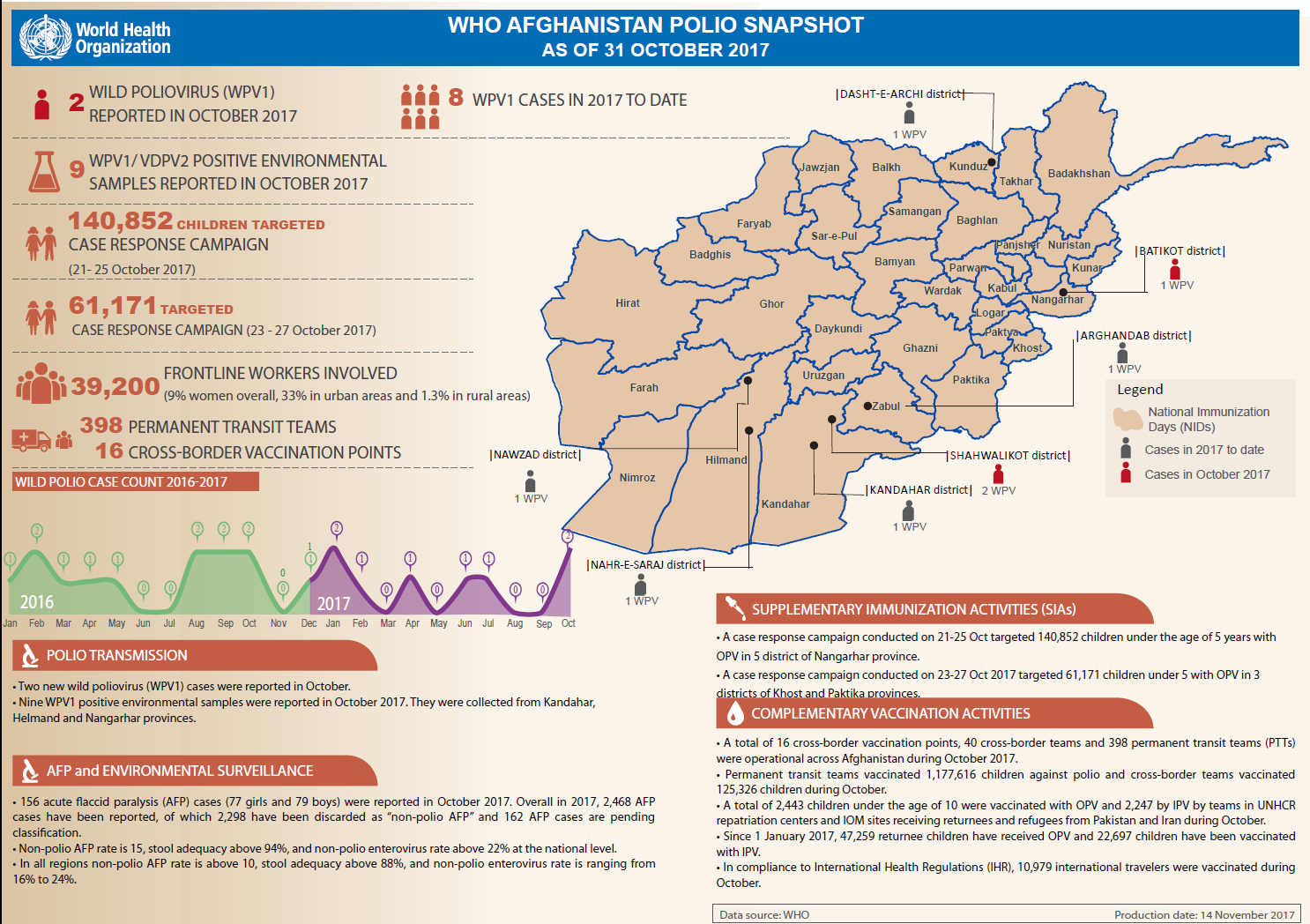
The Afghanistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Afghanistan.
In October:
Two new cases of wild poliovirus (WPV1) were reported, one in Nangarhar, and one in Kandahar provinces.
Nine new WPV1 positive environmental samples were reported in Kandahar, Nangarhar and Helmand provinces.
Over 202,000 children under the age of 5 were vaccinated in two different case response campaigns.
Permanent transit teams successfully vaccinated 1,177,616 children against polio, whilst cross-border teams vaccinated 125,326 children.